Similarly to the way this week went, I’m going to start this week’s blog by diving right into the details.
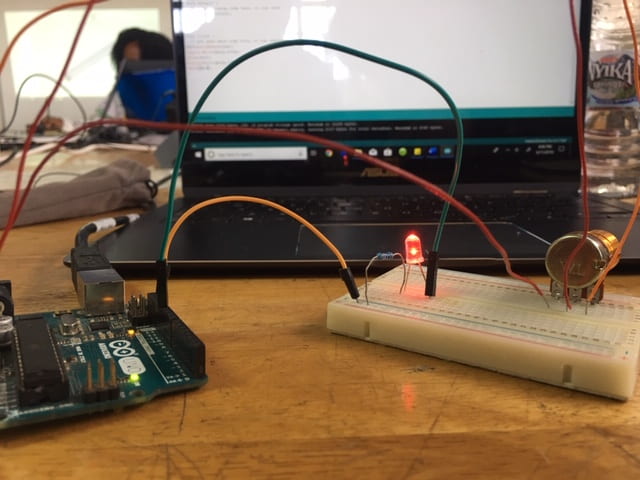
The first two days were focused on introductions and skills. We got lectures on the Engineering Design Process and Human Centered Design, and we broke into small teams to do a short, fun design challenge! This was my first time truly experiencing how clever and driven all these other interns are. They had ideas I could have never fathomed, and the whole experience was a lot of fun. On day two, we broke into groups to learn some skills we might need for prototyping. One group spent time learning about CAD and 3D printing, meanwhile I was in the group learning about Arduino and electronic prototyping. This might sound a little silly but as Andrew walked around and around our table explaining how microcontrollers work and how they fit in the context of an Arduino board, I could feel something that in that moment I could only describe as magic. I could feel everyone around me learning and growing and I could feel myself learning and growing alongside them and it was, just, magical.
Later that day, we got assigned our project teams! I’m on Team Suction and we’re working on a training model for nurses to practice the neonatal airway suction procedure on. My teammates are Nana from Dar Es Salaam Institute of Technology (DIT) in Tanzania, Foster from Malawi University of Science and Technology (MUST), and Chisomo from Malawi Polytechnic University (Poly). They’re all lovely and I’m excited to get to know them more during the course of this project.

Before this internship, I’d worked on four different design projects during my four semesters at Rice, but I’ve never had the opportunity to immerse myself as fully in a problem space as I did this week during our hospital visits. After being assigned to our teams on Tuesday, we were given the opportunity to spend Wednesday and Thursday at Mulanje District Hospital and Zomba Central Hospital. These visits really accelerated the first few steps of the Engineering Design Process, as we were able to speak to the users themselves in the environments where they would be using our technologies. In a span of 48 hours I went from never even having heard of neonatal airway suction to having heard five different nurses from three different hospital wards explain to me the procedures and common complications. It took weeks of research at Rice last semester to get this much information about OxyMon’s problem space, and we were able to accomplish this all in only two days thanks to these hospital visits.


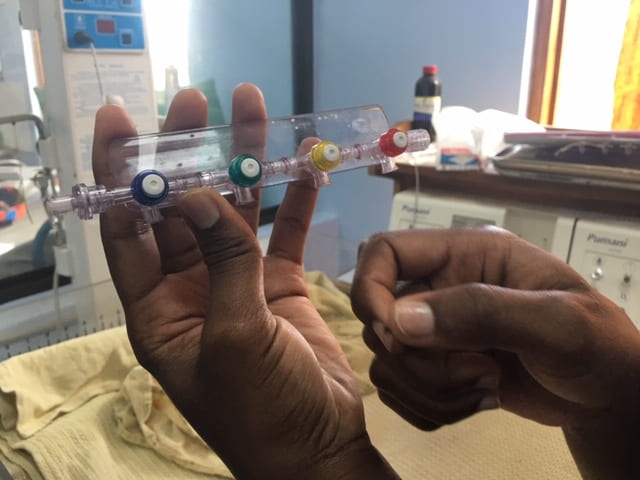
Speaking of OxyMon, I was able to utilize these hospital visits to get some information about oxygen concentrators to bring back to my team as we continue our work next semester. After having spent months researching the ways these concentrators are used and maintained in hospital settings in Malawi and working on prototype after prototype, it was the opportunity of a lifetime to witness the problem space and user environment live and in person. I was able to take pictures of concentrators being used in neonatal wards at Mulanje and Zomba, and I finally found out what types of splitters actually get used to connect patients (something that has been a pressing mystery to my team for many weeks). The most interesting part was our visits to the hospitals’ Physical Assets Management wards, or PAM for short. This is where technicians take broken devices to be fixed and where unfixable devices go to sit in what Rice 360 likes to call equipment graveyards. Dr. Bond talked to us about equipment graveyards at the very beginning of class last semester, and I’m having a hard time believing that I went from looking at pictures of broken equipment on a projector screen in the BRC in January to actually physically being here in Malawi, being the one taking the pictures myself. I won’t go into too many more details here in this blog, even though I’d love to write a whole report on my findings from this week (Nimisha keeps making fun of me, because apparently all I talk about are oxygen concentrators. I’ll spare you the same suffering she’s undergone as my roommate, listening to me talk about oxygen concentrators every day). Stay tuned for new iterations of OxyMon next semester, better than ever thanks to my time spent in Malawi!



Even though we’re done visiting Mulanje and Zomba hospitals, we are extraordinarily lucky to be positioned down the street from the Queen Elizabeth Central Hospital (QECH, or Queens). Our teams have access to Queens for the next several weeks as we begin prototyping, so we’ll be able to get all the necessary feedback. Next week, we plan to write a proposal of design criteria and present to nurses at Queens on Wednesday to ensure that we begin these projects with the correct direction in mind. For Team Suction specifically, we intend to find out exactly which difficulties of the suctioning procedure to focus our training model on.
Of course, we’ve being doing fun-stuff and life-stuff on top of immersing ourselves in our first week at work! Between the 11 of us living here at Kabula, we’ve split ourselves into mini teams to rotate the responsibility of cooking for our whole group each night. It feels like we’re having a big, family dinner every night on the deck at the lodge, and it’s a blessing to be growing closer to my fellow interns each week. My mini cooking-team made tacos last week. We persevered through a fridge that accidentally froze all our vegetables and the fact that all taco shells here are imported and unreasonably expensive compared to other foods. It ended up being a pretty successful meal for 11, all things considered!
We were also able to stop by a lodge at the bottom of Mount Mulanje on our way home from Mulanje Hospital. Some of the Malawian interns told us that some people believe spirits live at the top of the mountain. Apparently there’s a particular area on the mountain that people say not to hike under any circumstances whatsoever in order to avoid being taken by the spirits – people who go there tend not to come back. On the drive back, I saw that the top of the mountain was hidden by an eerie cloak of fog, and I could totally understand how one might feel that the top of the mountain might be home to malevolent supernatural beings.


Week one was truly a headfirst dive into life in Malawi and work during this internship. From meeting our teams to hospital visits to figuring out how to cook for 11 people every night, I feel so lucky to be learning and growing alongside so many wonderful, bright, caring young people.
