This week we finally got our projects and we finally got to meet the Malawian interns that we will be working with for the rest of our time here.
Day 12
Monday June 18, 2018
First impressions
Goals Accomplished
Meet new interns
Introduce projects
Share hospital observations
Review the engineering design process
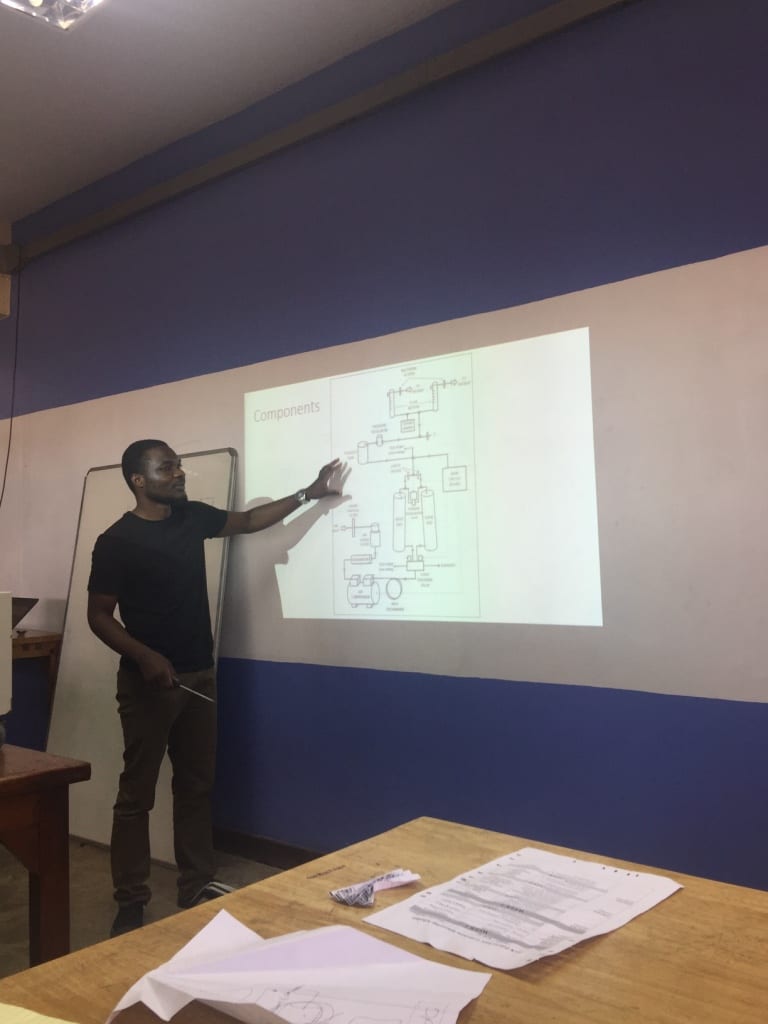
Today was super exciting because we got to the poly and met all eight of the Malawian students! Their names are Gloria, Alfred, Taonga, Isaac, Matthew, Demobrey, Nafe, and Timothy. We introduced ourselves, introduced our projects, and got a rundown of the engineering design process. We also had some fun activities like the airplane challenge, a scavenger hunt and lunch together at SPAR. I actually forgot how to make an airplane, but it eventually came back to me. It was a decent flight! Finally, we shared our observations from the hospital visits with the Malawian interns since they were finishing up their exams while we were visiting hospitals.
Scavenger hunt winners!
Day 13
Tuesday June 19, 2018
Teams!
Goals Accomplished
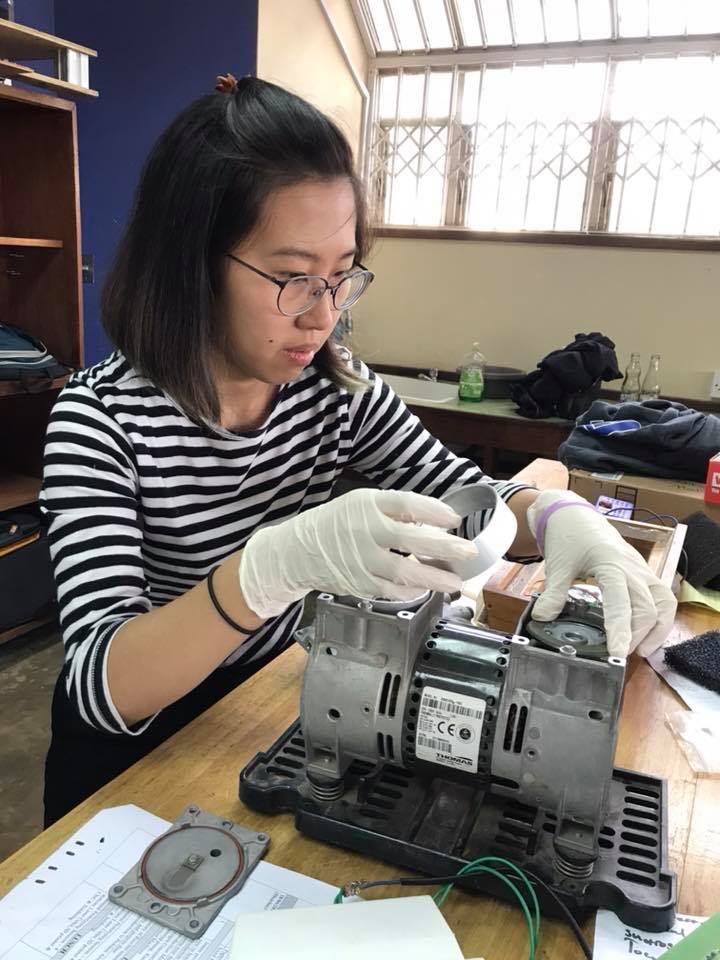
Learned about oxygen concentrators and suction pumps
Assigned projects
Assigned teams
We were split into four teams each with one Rice intern and two Poly interns. There are four projects that we will be working on including:
A continuous temperature monitor for mothers in labor
A device to turn off suction machines
A filter for oxygen concentrators
A procedure to reuse the chemicals inside of an oxygen concentrator
I will be working to create a device that turns off a suction machine (used to remove mucous/blood from patients). Often times the machine breaks when the secretion container overflows. The goal is to create a device that automatically shuts off when the container is full to prevent the machines from breaking. My team consists of myself, Taonga Tembo, and Demobrey Namaliya.
Andrew teaching us about oxygen concentrators
Day 14
Wednesday June 20, 2018
Arduino challenge
Goals Accomplished
Learned about microcontrollers
Today was really fun because we were all introduced to microcontrollers by Francis (design studio manager). We had many different tasks to complete using the Arduino Uno. The tasks included things like creating a thermometer using Arduino code and a thermistor circuit. We were all really proud of ourselves when we finished all of the tasks!
Arduino!
Days 15-16
Thursday-Friday June 21-22, 2018
Independent work
Goals Accomplished
Learned to use the CAD program at the Poly
Learned to use the 3D printers
Research about the projects we are working on
Thursday and Friday we had to create our own schedule since Francis and all of the Poly interns were very busy with their end of the semester projects. The design studio was busy with teams scrambling to finish their projects before final presentations on Saturday. We taught ourselves how to use the CAD program on the Poly’s computers, we did some 3D printing, and finally we were able to begin doing research on our assigned projects.
Day 17-18
Saturday-Sunday June 23-24, 2018
Into the wild
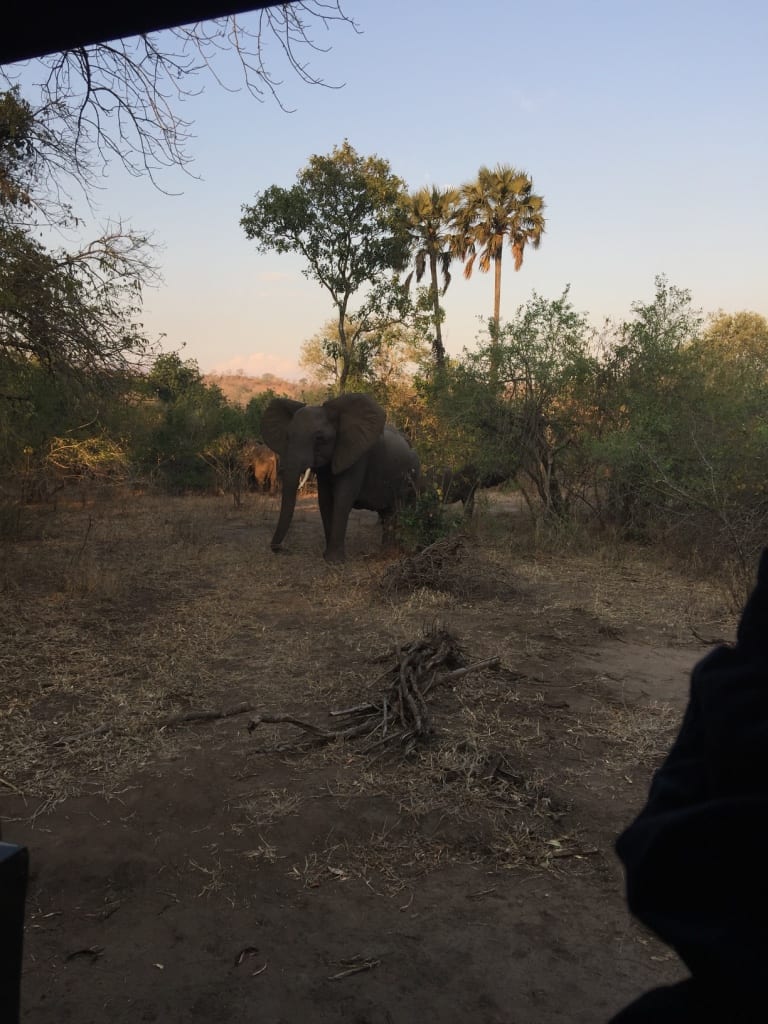
Saturday and Sunday we took a trip to the Majete game reserve. We saw some really cool animals including elephants, hippos, crocodiles and impalas!
We finally met the interns from Poly today! There are 8 of them, all finishing their fifth and final year here. It was really exciting to get to see who we would be working with for the next month. We did a bunch of introductory/get to know you stuff (like a scavenger hunt, which we placed dead last because we don’t know what a jigsaw looks like haha). But I’m really excited to start working on our projects with them!
Day 14
Francis and Andrew brought some broken syringe pumps and oxygen concentrators from Queens and we got to see how they worked. It was really cool because I had no idea how these devices were used. They opened them up for us and we got to look around and really get an understanding of how these devices may break down. A lot of the potential projects are based around syringe pumps (like a making a device that will stop the machine if the syringe pump starts to overflow with fluid) and oxygen concentrators (like an improved filter that will prevent dust from entering the machine).
We got our projects assigned today and I will be continuing to work on my temperature monitor along with Timothy and Matthews! We are all very excited to start improving the device, so I can’t wait to see the improvements in the next four weeks.
Day 15
We had a microcontrollers crash course today and I had a lot of fun! We learned a lot about how an Arduino works and we wrote some basic codes to turn on LED lights, display things, and read temperature with a thermistor. I really liked how hands-on everything is. I’m learning a lot thanks to Francis and Andrew for letting us play around with different things in the studio. And I think with a better understanding of the Arduino, I will be able to improve my code and my the temperature sensor more sensitive for my device.
Day 16
So the Poly students all have HUGE final projects that they have to present Saturday so they were all scrambling in the design studio to make them perfect. We didn’t want to get in their ways so we practiced using Autodesk Inventor, which is the program the design studio uses to create files that can be sent to the 3D printer. I am VERY bad at drawing, so I was happy to get a lot of practice. I made an elephant which I was very proud of. Maybe I’ll print it.
PS: We went to Mikos and got some ice cream and it was REALLY GOOD.
Day 17
I decided to work on my device some more, and I was pretty upset when I found that the IR is broken. And that was the ONLY IR I had on me. My device was reading numbers like 210 degrees and I am pretty sure that’s not correct. But I think the design studio has some extra IR’s, so hopefully we can use those and readjust our code depending on the model. We were also thinking of going back to a thermistor since they are way cheaper. A thermistor has a longer warm-up time than an IR, so our team back at Rice opted for an infared sensor instead. But I am hoping to do some more tests and see if I can reduce the time to warm-up a thermistor. Oh and today was very exciting because our sixth intern, Kristoffer arrived! So we have our entire team here in Malawi!
Day 18
We drove an hour and a half to the Majete Wildlife Reserve in hopes to spot some animals! We camped over-night (it was pretty nice, except it got VERY COLD) and went on three different safaris. We saw a lot of gazelle-like animals call Nyalas and we saw a family of elephants! It was really cool how close we were to them. We took a boat down the river in the middle of the reserve and saw a bunch of hippos! It was really amazing. Oh personally, warthogs were my favorite animals that we spotted. They are part of a group of animals called the Ugly Five which is rather unfortunate. It’s ok warthogs I appreciate you.
Hello! I just finished my first week working with the Rice 360 CPAP team. As the only non-engineer in the group (social policy analysis major), I am working with the Rice CPAP team at Queen Elizabeth Central Hospital while the rest of the group is mainly working at the Polytechnic University. There is a group of about 7-10 CPAP team members in the office and I am their intern for the summer.
I wanted to give a quick overview on what the Rice CPAP project is. A CPAP is a device that provides continuous positive airway pressure to help open up the lungs of an infant who is put on it. Often times, when infants are born premature, their lungs are not fully developed and they have difficulty breathing on their own. They can develop respiratory distress syndrome, birth asphyxia, or other conditions associated with lack of oxygen to the heart, lungs, and brain. In the US, these CPAPs costs thousands of dollars and are too expensive to be implemented in district and central hospitals in Malawi and the surrounding countries.
About 7-8 years ago a group of Rice undergraduates designed and prototyped a lower cost CPAP device called the Pumani to address this concern and after successfully creating the device, the Rice CPAP team started a clinical trial at Queen Elizabeth Central Hospital. The clinical trial was successful and 5 years later, the team has implemented the CPAP devices in all 28 government hospitals in the country as well as other partner hospitals and teaching institutions. They have conducted training visits to train nurses and clinicians on how to use the devices, do routine supply check ups, and also conduct supervisor visits to evaluate the nurses using CPAP.
The main project that I am working on this week is helping the team create a database and system for entering and analyzing data pertaining to the supervisor visits. When supervisors go to district hospitals, they fill out data sheets on how well the nurses are performing and using CPAP based on both qualitative and quantitative information. They must check whether the nurses are checking the infants vitals, whether they are correctly diagnosing CPAP patients, and other routine steps involved with successful CPAP delivery. They also evaluate the general quality of healthcare in the nurseries based on criteria such as the facility layout and the protocol for infection prevention.
I am working with excel as well as the raw data from these visits to create a system that makes entering and analyzing the data efficient. It’s been challenging but I am learning a lot from my main mentors, Sara and Sammy, about how to parse through large amounts of data and pick what is most important and be able to present that information most clearly and effectively. Out of my own curiosity, I am also able to read through the data on common conditions such as prematurity, respiratory distress syndrome, sepsis, and birth asphyxia that affect newborns and do my own reading and learning about how they are addressed here in Malawian hospitals.
After a busy and exciting first week, we spent the weekend at Majete National Game Reserve on a safari. We were able to do an afternoon/evening safari where we saw a beautiful sunset, a morning safari as the sun rose, and a boat safari along the river with hippos and crocodiles. The best part was finally getting to see elephants (my favorite animal in the world), especially the baby elephant with its mama. They are so calm and peaceful. Looking forward to more adventures here and to continue on with my project!
It’s been such an exciting week! Besides visiting Majete Wilderness Reserve and seeing some elephants up close, we finally met the six other interns from the Polytechnic who we will be working with over the next month. Most of them are electrical engineering majors with a few mechanical and telecommunications majors in the mix. They’re such a friendly bunch of people and they have some really interesting projects. One was converting wind energy from moving automobiles into electrical energy. There was even one project with a mechanical self-flushing toilet.
Picture with Alfred and Nafe, two of the Polytechnic interns, during a scavenger hunt.
Much of this week was spent as an introduction course to the skills we will be needing in the next few weeks. We spent quite a bit time going through the function of the oxygen concentrator and suction machine. Both devices are quite complicated with many parts but breaking down the functions into the individual parts helped me understand what we were working with. We also reviewed Arduinos and basic programming skills.
We were also introduced to the different projects that we will be working on. I’ve been assigned to work on sieve bed regeneration for oxygen concentrators. The two sieve beds in oxygen concentrators work to trap the nitrogen from the pressurized air that passes through, leaving behind around 90% oxygen that goes to the patient. However, due to moisture that may enter the oxygen concentrator, the sieve beds become damaged and need to be completely taken out and replaced. Spare parts take a long time to wait for which makes regeneration of the zeolite in the sieve beds necessary. There are a few possible designs that may work, both mechanical and electrical. I’m excited to try and figure them out with the two other interns on the team, Nafe and Isaac.
This week was exciting and eye opening. Our time was spent presenting our technologies at the Polytechnic school of engineering (the Poly) and visiting the different district hospitals in Malawi. Visiting the district hospitals definitely helped us to see how we fit into the big picture (of improving neonatal and maternal healthcare) and how we can help with our technologies.
Day 5
Monday June 11, 2018
Getting Started
Monday was a long, busy, and fun day at the Poly. We made new friends and colleagues and I met up with some old friends as well!!!
Goals Accomplished
Present our technologies to students and administration at the Poly
Meet students and staff at the Poly
Reunited with old Malawian friends!
We arrived at the Poly at 8 am (our usual time) and immediately began preparing our technologies for the mini showcase that was happening today. Dean Reggie, Dr. Kortum, Dr. Oden, John (A Rice Alum) and others from the Lemelson foundation were visiting to see the work that Rice 360 is doing. It was a lot of fun to be able to show our projects to the Rice 360 visitors and to see the amazing work being done by the students at the Poly as well.
Presenting the Cervical Cancer Training Kits!
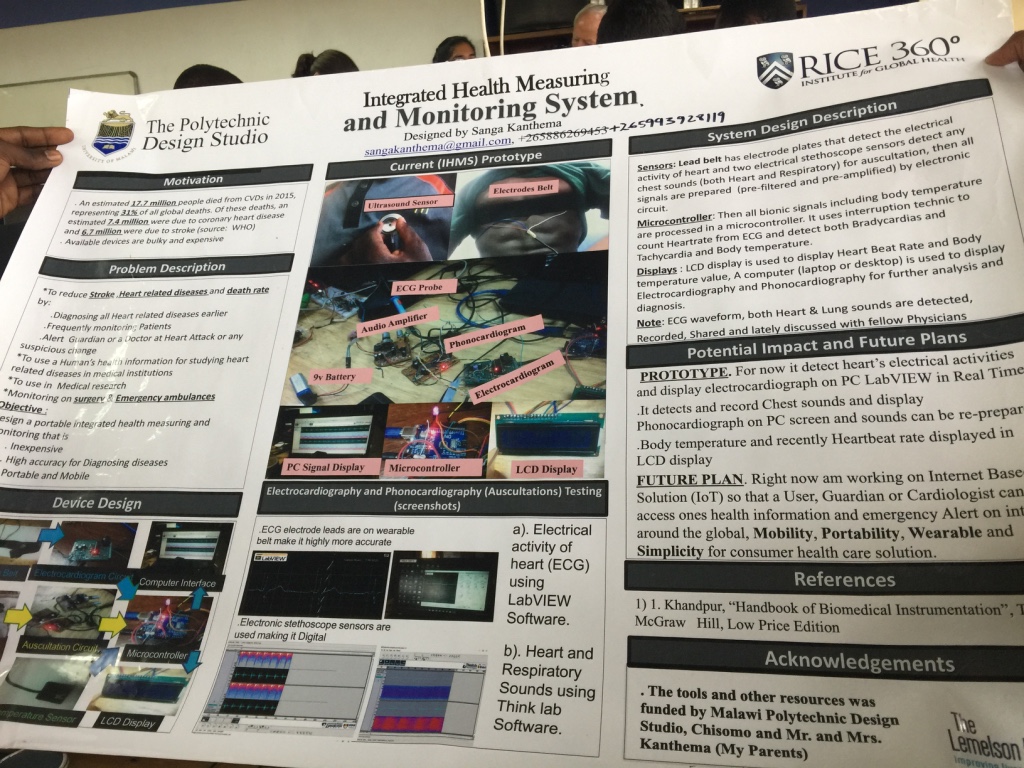
We met so many amazing people. We met a team that was working on making a drone from scratch. I also met Sanga, a guy who made a health monitoring system (mostly an ECG using a microcontroller) from scratch! (Notice that I didn’t say a student) Sanga isn’t actually a student at the Poly! He apparently just showed up one day with ideas so the design studio at the Poly just adopted him and he ended up winning their design showcase!
The team making a drone from scratch!Sanga and his ECG project!
After the presentation of the technologies, we had a great lunch and I was able to catch up with some of the Poly students that I had met in Houston two summers ago. The Cervical Cancer Training Kit Project that I have been working actually began that summer with the Malawian interns. It was such an amazing moment because I had promised them that I would visit them in Malawi. We reminisced on our time back in Houston and made plans for hanging out in Malawi!
A great lunch at the Poly!Hilary, Me, Chimwemwe, Waheed, and Borgestein reunited!!!!
Day 6-8
Tuesday-Thursday June 12-14, 2018
Staying Optimistic
The rest of the week we split into two groups and visited four hospitals. Angela, Franklin and I traveled with Jossef, a lecturer at the Poly. Akshaya and Sajel traveled with Prince (a nurse at Queens), and Andrew (staff at the design studio). The visits to the hospitals were eye opening, humbling and motivational. Despite the lack of resources in these hospitals, the staff are so hardworking and are doing their best to keep mothers and babies alive. They were also very welcoming to us and open to collaboration for the development of devices that could help them out.
Goals Accomplished
Visit four district hospitals (Zomba, Mulanje, Thyolo, and Queens)
Observe the Neonatal and Maternal wards at each of the hospitals
Receive feedback on our technologies from hospital nurses and staff
Identify areas of need in neonatal and maternity wards
Bring back potential project ideas to improve the neonatal and maternal wards
On Tuesday we visited the Zomba District Hospital. The first hospital visit was definitely the hardest. We first visited the neonatal ward then the labor ward. What we saw will stick with me forever. As we walked into the NICU (something that we would probably never be able to do in the U.S.) we saw around 20 babies in a hot room (since there were no incubators, the entire room was kept at a high temperature). Many of the premature babies were sharing a small heated bed (meant for only one baby) and were receiving oxygen from an oxygen tank. In the labor ward, the “rooms” were separated by curtains and we could hear some of the mothers in labor as we were talking with the nurses. It was a very similar situation at each of the hospitals that we visited. There were so many differences between these district hospitals and any hospital I’ve ever been to before.
Multiple babies sharing one bed and a radiant heater
At first, it was difficult to process so much information at once. We observed so much that could use improvement. As we asked the nurses about the resources they had, we began to see many deep rooted problems that were out of our control. For example, the shortage of nurses was a huge problem which was caused by lack of funding. Many babies are dying at night because there is only one nurse watching both the labor ward and the neonatal ward. Additionally, the power outages (caused by an unstable power grid) often leave babies without life saving heat and/or oxygen. At first, the future seemed grim without the availability of these resources. However, there is definitely a lot more that can be done to help. It was inspiring to see that the B-CPAP machine (donated to these hospitals and designed by Rice 360) was already making a huge difference in many of the hospitals and saving babies’ lives. This helped me stay optimistic. I am motivated to help in any way possible.
With help from the nurses and hospital staff we were able to understand what problems the hospitals are facing and the causes of these problems. I took many notes on the conditions of the hospitals and the questions that were answered by the nurses.
Key observations
Infant and maternal monitoring is difficult with low number of nurses
Patient temperature is a key indicator of their condition and needs to be monitored more often
Heart rate is also a key indicator that is not monitored very often
Low nurse to patient ratios makes it very difficult to monitor any patient at a regular basis
Dusty, humid and high temperature conditions as well as power outages affect the function of medical devices designed for use in other countries
Many oxygen concentrators (provide oxygen to patients) break because of the dust in the air
Many devices are fried through power surges
Many (almost all) medical devices are donated and (e.g. incubators, syringe pumps, oxygen concentrators) end up broken
Many nurses don’t know how to operate the devices and don’t have time to learn so some devices end up completely unused
There is no standard for the devices that are donated (There are many different brands of the same device and they all operate differently)
Many of the devices that are used, aren’t used properly (no training or manuals) so they break.
Once the devices break, they can’t be fixed because the spare parts are not manufactured in Malawi and they can’t order 10 different spare parts for 10 different devices of the same type (e.g. there are 10 different kinds of filters for oxygen concentrators because there are 10 different brands)
The hospitals are dependent on donations of certain non reusable medical products and medical devices (e.g. glucosticks, feeding tubes, syringes) that aren’t manufactured in Malawi and often run out
Education surrounding preventable diseases is helpful
Diseases such as cervical cancer, hospital acquired infection, or infant pneumonia is preventable if people are informed on the causes and on preventative measures
Broken oxygen concentrators in the physical asset management (PAM) aka the “graveyard”
We hope that with this information we can make devices that can alleviate some of the difficulties that nurses are facing in the hospitals. I especially want to create SUSTAINABLE devices that are fit for the environment and users (cultural differences must also be accounted for) in these hospitals. I especially want to focus on education because it is a key factor in prevention of many diseases.
Day 9-11
Friday-Sunday June 15-17, 2018
Eid Mubarak!
We had a long weekend because 30% of Malawi is Muslim and Friday was the end of Ramadan! We spent the weekend visiting the markets, walking around and getting to know our neighborhood. Friday we went to the Blantyre market and to Veg delight (an Indian restraint in Blantyre). Saturday we went to Limbe Market and bought fruits and beautiful cloths. Today (Sunday) we plan on watching the Germany vs Mexico World Cup Match!!
“So, tell me more about Hinduism and how your family practices it”, Mikah asked me as we were both struggling to cut a piece of bone chicken with a fork and knife. Startled, I sat back in my chair for a second. A young college student like I, Mikah and I met at the Rice 360 faculty and student dinner in my first week here. He explained that he was religious but admitted that it is often difficult to practice when he is away from home and something that he wishes he could better at. I was surprised at how this fellow student who I had just met maybe 30 minutes ago was able to ask such insightful questions that delved beyond the usual academics and college life. We went from talking about religion and race to discussing how we both deal with homesickness during the semester. There was a refreshing depth and complexity to our dinner conversation that I was beginning to see in many of my interactions with the Malawians and Rice 360 staff here. I realized just how humble all of the Malawians I have interacted with are and how comfortable they are with the idea of imperfection. They are able to open up about their own vulnerabilities. Back home, I have noticed how rooted our culture is in chasing perfection and we have a hard time facing our shortcomings. It is inspiring to be able to observe and I hope I too will able to delve into how I perceive myself and others and be more confident in discussing weaknesses and areas of growth.
As the week went on, I was cognizant of this phenomenon at the different district hospitals we visited. In Malawi, there are two large central hospitals: Queen Elizabeth Central Hospital in Blantyre where we are and Kamuzu Central Hospital in Lilongwe, which is the capital city about 4 hours away from where we are. These hospitals are where the most complicated surgeries, deliveries, and cases are seen and where a very small percentage of the population ends up going. Surrounding these central hospitals, there are district hospitals. These district hospitals are smaller in size, have fewer human and capital resources, and where most Malawians go if they have a serious health concern. When we visited district hospitals, we focused mainly on the maternity and the nurseries as the wards we wanted to talk to the nurses and staff in and gain as much insight into how they deliver healthcare. These district hospitals rarely have even a single MD so nurses and students end up taking on many of the duties that a doctor would perform back in the US. We asked the nurses on staff questions and wrote down as many things as we could keep up with.
I again noticed that these nurses had a depth to them that is not only hard to come by and but also difficult to uncover in the US. After having only met them for 15-20 minutes, they were able to open up to us about the hardships of healthcare delivery in Malawi. For example, in the labor ward, where protocol states that nurses should check the fetal heartbeat during labor every 30 minutes, when there are only 2-3 nurses for the entire labor ward who must perform deliveries, check all the mothers vitals on a rotation and all of the infants vitals on a rotation, they have a hard time doing everything. In addition to the lack of human resources, they explained that they do not have a working electronic fetal doppler to check the fetal heartrate during labor and so they must use a manual one which is harder and more time consuming to use.
Issues like these were common among all the maternity wards and nurseries we visited and while it was hard to see their hardships and I ended many of the visits to the district hospitals feeling somewhat defeated, seeing the raw truth of healthcare here and its successes and weaknesses was so important. I could not be more grateful to the nurses and students who took time out of their already busy schedules to answer our questions without a single complaint. They always did so happily and did so honestly. I am so excited to continue learning and digging deeper into the stories of the nurses and people here.
Sajel and I visited our third and final hospital in Zomba, which happened to be a central hospital rather than a district hospital. In fact, Zomba is the first central hospital built in Malawi. A lot of the older, more worn down parts of the hospital were built in the colonial times. Zomba was also the very first nursing school in Malawi, and Prince said he came to Zomba to train during his nursing school days.
In the nursery, we saw many of the same problems as in Thyolo and Mulanje.
There are 30-40 infants, but only 3-4 nurses on duty. This is common in all the hospitals we’ve visited, so it makes it so difficult to test vitals and constantly check on the babies.
We saw a continuous monitor in the corner of the ward that tracks temperature, oxygen levels, and pulse. However, it was broken and the spare parts were not readily available, so the nurses couldn’t use it.
Sajel and I saw a baby being treated with gastroscesis there. I never saw an actual case of gastroscesis until that moment and it was truly eye opening. The nurse told us that since Zomba was a central hospital, they were able to treat gastroscesis. However, they didn’t have the special plastic gastroscesis bags (just like in the previous hospitals), so they used gauze also to cover the intestines prior to surgery.
We met Daniel at maternity and he told us that the most challenging aspect is checking for contractions. Ideally, the nurses try to check for contractions every hour by feeling with their hand and checking the amount of time between each contraction using a stopwatch. However, there are sometimes only 2 nurses for over 20 patients every day, and it takes at least 10 minutes to do this measurement. Daniel was really excited to talk to us because he is a huge advocate for maternal health. Every year he hosts a walk from Blantyre to Lilongwe (which is over FOUR HOURS AWAY by CAR). The walkers will stop at various locations and host events and talks educating people on maternal health! It’s such an amazing initiative and I’m excited to have gotten his contact information so I can learn more about what him and his team do!
Visiting PAM at every hospital was equally discouraging because it was like a graveyard for donated medical equipment. There were oxygen concentrators (which are so important for babies with birth asphyxia), syringe pumps, constant monitoring systems, and so many other devices that could be used in the wards but aren’t because they are broken. These devices may last for 6 months to a year, but then break down. Since these devices are donated from all over the world, it is difficult to order parts and components. And there are a ton of models for all the devices, so it is both expensive and inefficient to order components for all these different models.
Often times, these devices are donated with no user’s manual, so nurses and staff are not properly trained on how to use the devices. Furthermore, PAM workers are unsure of how to fix these devices. It’s so frustrating seeing this because sustainability is so important when it comes to medical devices. They can’t be donated without proper training to both the nurses and PAM workers and access to parts. Otherwise these devices will be unused and gaps will still exist in hospitals like Mulanje, Thyolo, and Zomba.
Day 9
We went to Queens today for a second time, and after visiting the district hospitals, I was able to see a lot of overlaps. Although Queens is one of the primary hospitals people are referred to, there are still some gaps. For example, the nursery had about six different syringe pumps, but none of them were being used because they were broken. And only two out of the six or so radiant heaters were working. For the most part, kangaroo care is heavily depended on (just like the other hospitals we visited).
And the PAM area was HUGE. There were rows and rows and ROWS of devices. It was bigger than any other site.
The PAM specialist told us that if the parts are available, they could fix devices in under an hour. But because parts are really hard to get, they are just holding the devices there. Some of the machines like the oxygen concentrators have been there for 2 years! We even saw an entire MRI machine 😮
Day 10
LAUNDRY DAY. Once again, I added too much laundry powder. Now, my pants are going to be crunchy like a chip.
Day 11
We drove out to Limbe today and visited the market there! It was HUGE. There were so many stalls lining the busy road, people yelling and bargaining for things. There were A LOT of shoe stores haha. I ended up buying really pretty cloth called a chitenja, and people use them for swaddles, dresses, and other things! I can’t sew but I’ll figure out something to do with it.
“Eventful” doesn’t even begin to describe this week. On Sunday night we had dinner with Dean DesRoches, some of the Rice 360 team, and the Malawian interns who will be coming to Houston in September. It was such a great opportunity to meet some of the engineering students from the Polytechnic and compare their projects and interests with ours. What seemed even more amazing was hearing about the various projects that have been going through the design studio. Everything from an infant monitoring device to an autonomous drone was presented on Monday. The students’ ingenuity and work ethic were so admirable, and I felt that I learned an incredible amount from hearing about their design process.
Our focus this week revolved around needs finding at the big district hospitals. Our stops included Zomba Central Hospital, Mulanje District Hospital, and Thyolo District Hospital. Within each hospital, we went to the maternity ward, nursery, and labor ward to speak with the nurses and discuss some of the current issues they face daily. The wards were a completely new experience to me, something that I could not have truly imagined. The concept of “limited resources” has never been as clearly encapsulated as seeing three infants huddled together under one radiant warmer, trying to escape the all too real threat of hypothermia. Often the hospitals had one or two heaters for the entire room but no way of monitoring or controlling the temperature consistently. Even getting constant electricity is a struggle. The hospitals have to depend on solar power and backup generators, and when those sources of power fail many processes come to an unwilling halt.
Solar power panels at Thyolo District Hospital, some of the most reliable ones we saw
I honestly don’t even know where to begin with describing the technology. Much of the equipment around the hospitals was donated, which in theory seems beneficial. However, the models of the donated machines are completely different. When a machine breaks, the Physical Assets Management (PAM) has to face sometimes more than ten different models of the same equipment and figure how to fix them. The wait for spare parts is even worse because they often come from overseas and may take several days to arrive.
PAM at Zomba Central Hospital. Most of these machines are waiting for spare parts.Different models of broken oxygen concentrators at Thyolo District Hospital.
One example we saw of this was in the oxygen concentrators. Each hospital had at least five different models, with each requiring differently shaped filters. Expecting technicians to understand all these machines from user manuals and be able to fix them is an impossibility, but one that many hospitals must have to keep operations running.
The nurses at the hospitals are some of the most dedicated people I have ever met, considering their work load and environment. Regardless of day or night shifts, the staff is stretched thinly over several patients and even several wards. While the tangible difficulties facing district hospitals is overwhelming, there seems to be underlying about personnel. The incentive to study and work as a nurse in Malawi seems low. That’s why I’m even more glad to see the level of care the nurses have when taking care of the infants and mothers.
At a dinner recently, Dr. Leautaud posed a question to us: “What do you want to be when you grow up?” In theory this should be simple to answer. From the time we’re in kindergarten, we think about the time when we will be adults. I used to be stuck at this question, knowing my interests but unsure of why I was interested. After this week, however, when I think about what I want to do “when I grow up” I think less in terms of jobs or roles. Instead, I think of the nurses and doctors at the hospitals, of the student innovators and the lecturers who support them, of the researchers studying disease prevention. It’s their dedication to their work that I want to remember and embody.
We split our group up into two teams and ventured to some district hospitals today (we always move in a pack so this was the first time we separated). We planned to focus our visits on three aspects of the hospitals: the nursery, maternity ward, and PAM (physical assets maintenance area or the place where hospital staff send off broken medical equipment). Prince, Andrew, and Jeremy (a bioengineering student) first took me and Sajel to Mulanje. I thought Queens was different, but the Mulanje district hospital wasn’t like anything I’ve ever seen.
The hospital in Mulanje was about an hour and a half drive from Blantyre. We drove up a winding hill and reached the hospital, which was at the base of Mount Mulanje. The clouds were so close I thought I could touch them. The hospital was much smaller in size compared to Queens because Mulanje is a district hospital. Prince explained to us that there are three levels of medical care people can receive. People will first go to small local health centers, which are spread throughout all districts in Malawi. The health centers have midwife technicians and medical assistants, but no clinicians or doctors. If the condition is too severe, people can be referred to the next level of care at district hospitals. They are larger and have one clinician, a registered nurse at every ward, and interns. These district hospitals are better equipped at handling more serious conditions, but may not have specialists or general surgeons. As a result, people may then be referred to the final level of care at central hospitals (such as Queens). Prince told us that it is important that the earlier levels of care are improved as this will reduce the amount of time people have to spend untreated. If people have to be constantly referred, they will spend more time travelling to far off hospitals and risk making the condition more serious.
Our first stop was the nursery. We walked into a small room with cots lining the walls. The registered nurse greeted us before we asked her some questions about the infant ward. We talked A LOT, but I’ll only cover a few of the things we discussed:
The registered nurse told us that power outages were extremely common. Although they do have backup power via solar energy, this only lasts about an hour before running out. Babies with hypothermia who are placed under the radiant heaters are at risk and must be put in Kangaroo care (warmed by their mothers’ body heat). As a result, hypothermia is a leading cause of infant mortality at Mulanje
Birth asphyxia is another primary cause of infant death at Mulanje because there are no available oxygen concentrators.
Gastroscesis (a condition where babies are born with their intestines outside of their body because of a large opening at their stomachs) is very common. But these babies are sent to the central hospital. Plastic gastroscesis bags to hold and protect the intestines are not available, so the babies intestines are covered with gauze as the baby is transported to Queens. This is very dangerous, however, because the gauze absorbs moisture from the intestines, destroying them. Sajel showed her prototype gastroscesis bag to the nurse and she got some great feedback!
After thanking the nurse at the infant ward, we moved on to the labor ward. It was very busy when we visited, so we couldn’t spend very much time there. It was so crowded, in fact, that all the beds were taken and patients had to be treated on the floors.
Thermometers are not available (because they break down or are missing), so nurses have to check the temperature of mothers using their hands. Fever is extremely common because of malaria births, so lack of thermometers is a huge problem (I was also able to briefly show them my prototype and the feedback I got was extremely helpful!)
The nurses use the metal fetal heart beat scopes to check the status of the fetus during labor. There are only a couple and with over 30 patients being seen every 24 hrs, it can be difficult to constantly monitor the fetus. I looked behind me and noticed a box of 4 or 5 fetal monitors and I asked why they weren’t used. The registered nurse told me none of them were working and that no proper training was given when the devices were introduced at the ward. Prince told us that checking the fetus is crucial because if they notice something wrong, they can take immediate measures. But without knowing how the fetus is doing, labor may be prolonged. As a result, birth asphyxia is a common condition there.
We drove another hour and went to the much larger, much newer Thyolo district hospital. Thyolo sees almost double the number of patients as Mulanje, but there are almost the same number of nurses still on duty. As a result, constant monitoring for the patients is quite difficult. There is a high rate of birth asphyxias as a result of fetal distress during labor (due to the inability to continuously check the status of the fetus). Gastroscesis is also a common condition seen by the nurses, occurring about once every month.
What stood out to me most on our visit to Thyolo was something the registered nurse at the infant ward told us. She said that the members of the CPAP team for Rice 360 were their only suppliers for supplies like oral gastric tubes and suctioning tubes. If the CPAP team were to stop visiting the hospital, Thyolo would lack a sustainable supplier for these medical equipment. This was really shocking to me because without these devices, it is very difficult to provide oxygen for babies with birth asphyxia and nutrition for premature babies who lack the correct reflexes to feed.
This past week has been busy and all over the place, but not in a bad way. Early in the week we presented the device prototypes we brought from Rice to Rice 360 staff, students at the Polytechnic working on medical devices themselves, the Rice Dean of Engineering as well as USAID staff! We got amazing feedback from everyone there and people loved the work that was being done. My favorite part was learning about the projects being developed there, some examples were central patient monitoring systems for hospitals, phototherapy lights for jaundice in newborns and more. A very interesting project I hope to work with a bit more that was being developed at the Polytechnic was an autonomous drone that can be used to deliver food to remote villages with little access to food. The students built the entire drone from scratch. It is very inspiring and motivating seeing students at the Polytechnic build and design these devices, they most often have less resources than we may have at Rice but build such novel and impactful devices, it really shows me how your work is really dependent on your ethic and not your situation.
Later during the week we visited district hospitals, which are smaller hospitals that are government funded and closer to villages. The standard of care at these locations is enlightening, they sometimes use technology that to a westerner is outdated and sometimes old fashioned but is the norm in these locations. A lot of the problems they face in caring for the patients are simple to fix, but only in theory, such as more tools to monitor patients. But the underlying issue is that this costs the hospital a significant amount of money that they sometimes do not have. We did see the Pumani bCPAP devices in each of these hospitals being used actively! This device is incredibly helpful for infants with mild to severe respiratory problems. The nurses love the machine and it is nice to see the impact it has on the patients. The visits to these hospitals makes me glad that I am part of the Rice 360 team working to design low cost devices aimed at ending preventable deaths.
These visits also showed me how important it is to make implementation and training an integral part of introducing a device into a clinical setting. This is something that was not very obvious before but after visiting nursery and maternity wards is very apparently important.
This coming week we will begin our work with our fellow interns from the Polytechnic, I have been looking forward to this for a long time and it is about to begin! I think the projects I’m most interested in are the central patient monitoring systems and the autonomous drone delivery device.