As I prepare to talk about the Chitenje Warmer, I’m having to reconcile the work I did with the results I got. The warmer didn’t pan out, and it ended up not being an effective tool. What I’m struggling with is whether that means we reconsider how the device was built or fundamentally shift where we approach the problem of neonatal hypothermia? Do we try and fix something that we’ve built or focus on building a new device?
As a student, failure stings a little, but failure is another opportunity to learn.
“Be resilient.”
-Dr. Leautaud, Rice 360 Internship Interviews
Even though this device doesn’t work, the experiences I had working side-by-side with the nurses and physicians in Queen Elizabeth Central Hospital become no less meaningful on both a personal and educational level. I’ll talk about where the device failed, and I’ll talk about my recommendations for it moving forward. I’ll speak about the tenacity I saw in the operating theater to do right by the patient, and I’ll speak about how ready those nurses were to learn how to use a new device.
As I continue to pursue global health, I know that the road ahead will be filled with successes and failures and that every step will hold a new lesson.
Our two months are nearly up. When we arrived, two months felt like a fair amount of time to work here at the Poly. Right now though, I feel I blinked and found myself at the end. I can’t believe that the morning breakfasts, struggling to funnel 8 people out the house, and the walk from the front the of Poly to the design lab are all coming to an end. We’re currently preparing our final presentations, and it’s crazy to think that this marks the end of our internship.
I’m learning a lot about what goes into implementing a device in a real-world setting, but as an engineer, we have to be critical of what we’re implementing. There are definitely some design characteristics that we need to go back and reconsider with the Chitenje Warmer. For the last few days, the efficacy experiments I’ve been running have been providing me with a fair amount of raw data (tracking usage, heat transfer, etc.) that I’ll need to go back and analyze. Whether this device ends up being a success or is proven to be unsuccessful, working with this device gave me a chance to work with a part of the design process I hadn’t seen before. We’ll see what results the data holds!
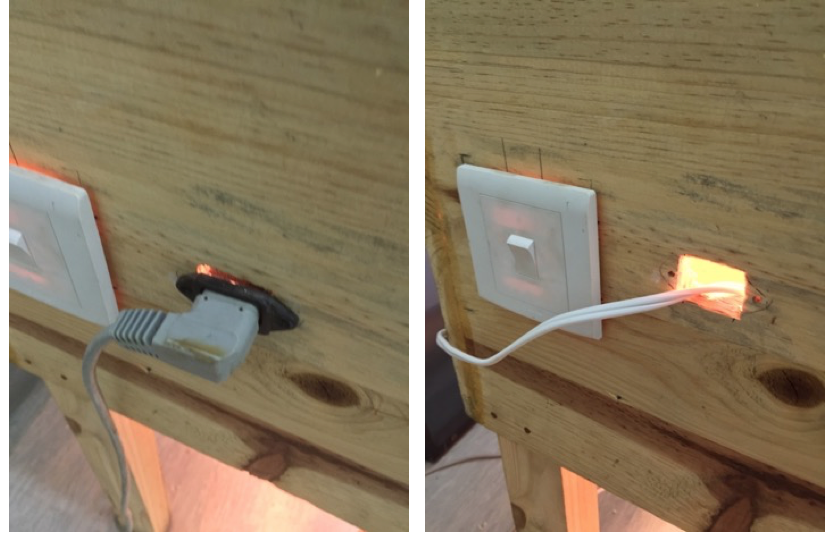
One of the first things we realized with the Chitenje Warmer was that a temporary power cord wasn’t going to work. When we found it the first time around, the device had been missing its power cord, so our solution in this case was pretty straightforward. We made and installed a permanent power cord into the device. This way the device’s functionality wasn’t dependent on an external power cord.
Installing a Permanent Power Cord
Once we overcame the technical barriers, the next step was to relocate the device so that it could better serve its target population (neonates delivered via c-section). Upon the advice of Dr. Meja, we moved the device to the labor ward operating theaters. Once we got it into the theaters, we had to figure out how to integrate the device into the nurses’, physicians’, and midwives’ workflows.
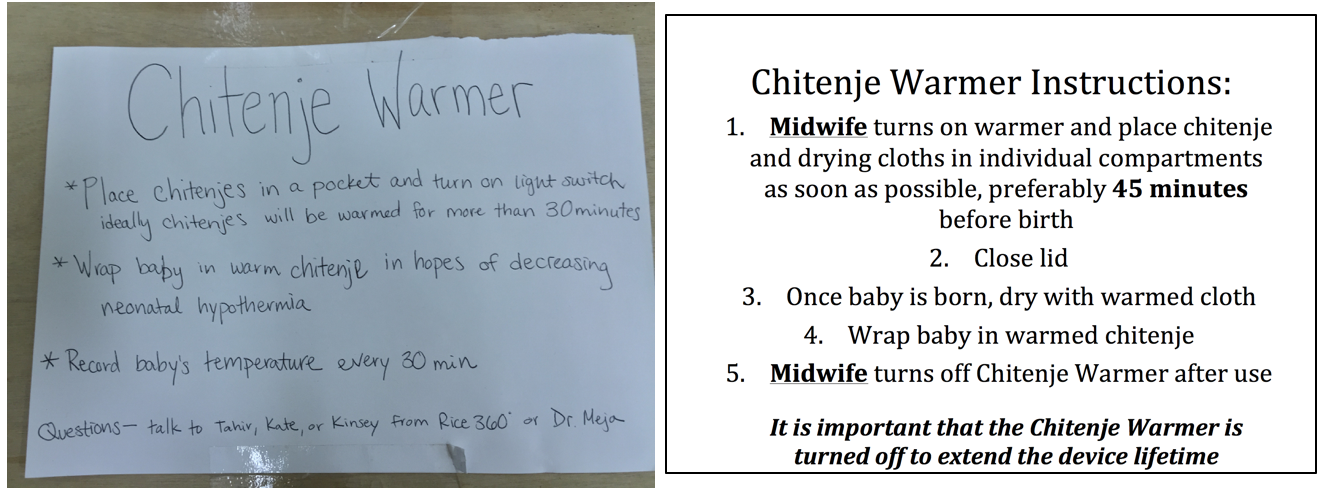
A Passive Set of Instructions
By itself, the device was wooden box with an on/off switch. We needed to add labels and instructions so that the nurses and midwives who’d be using the device had some sense for what it was they were using. We drafted up a set of instructions, and I sat in the breakroom for a bit, showing the instructions we had drafted to a few of the nurses.
“Someone needs to be in charge of the device.”
-Nurse, Labor Ward Operating Theater
After a little while, we had a clear idea of what our instructions needed to look like. For sure, the instructions had to include which set of healthcare provides (the midwives) would be in charge of using the device and turning it off when it wasn’t in use. The passive instructions we wrote were only part of the picture. I also actively oriented nurses and midwives whenever I could in terms of how to use the device.
Active Orientation
Part of this meant waiting in the break room, walking with nurses to where the device was being used, and asking if they had seen it before. A fair amount of the time I would find the midwife before the c-section was started and ask them if they had seen the device yet.
Overcoming the technical challenges, designing a set of passive instructions, and orienting nurses and midwives was a part of the design process I hadn’t seen before. As a student engineer, I’ve often gotten to the prototyping stage, but this was the first time I was working to implement a device inside the hospital. It’s hard to appreciate the nuances involved with human factors until you’re actually trying to get a device up and going in its intended setting. Even now, there’s still so much to do, but we’re getting there little by little!
We tackled the challenge of neonatal hypothermia from two sides. The first side involved designing a few different monitoring systems to alert physicians and nurses of a neonate’s thermal condition (hypothermic, normal, or hypothermic). The second side was to look into a device that was built by last year’s interns.
Last year’s interns had built a device known as the Chitenje Warmer, a device meant to warm chitenjes (cotton blankets brought into the hospital by expectant mothers). Typically, once the baby was delivered, it was placed on the mother’s chest so that the mother’s body would warm the neonate. This warming technique was known as Kangaroo Mother Care (KMC). The reason this device was made was because mothers who underwent c-sections didn’t have the strength to provide KMC to their neonates. The Chitenje Warmer was meant to act as an indirect substitute for KMC.
Last year, the team was able to build their device, but they weren’t able to implement it in Queen Elizabeth Central Hospital (QECH). That’s where we came into the picture. We had to figure out why this device wasn’t being used in the hospital. At the same time, we looked into the device’s efficacy.
It’s hard to imagine that a project that started in a classroom back at Rice made it all the way to the the hospital halfway across the world. 5 months ago, we had an idea, and today, Christine and I demonstrated to Dr. Kommwa, Dr. Meja, and the others at Queen Elizabeth Central Hospital how we made that idea into a reality. We should’ve been nervous, standing in front of a room full of doctors, but I was excited. I was excited to talk about we had built and to learn about what else needed to be done to our device, the PneumaShoe.
Standing in front of them, we had to make sure our explanation was tailored for the doctors who sat before us. They didn’t want to know about the Arduino, the long hours debugging it, or the circuit components. They wanted to know about how it would be used, which patients it was meant for, its price, and its maintenance. Once we had convinced them of the device’s worth, they wanted to know about the human factors involved.
“The motor’s a little loud.”
-Medical Student
The motor he was referring to clattered against the device’s wooden frame. In our defense, it wasn’t ear-shattering, but we had already brainstormed ways to muffle the sound.
“Can you add wheels to it? What about some lights so that we know it’s working?”
It all came back to human factors. They started making suggestions to improve its usability within the hospital. They wanted it to be smaller, quieter, easily moved from patient to patient. The surveys we passed around eventually made their way back to us with a variety of results – all food for thought once we got back to the Poly.
“Venous thromboembolism (VTE) is the leading preventable cause of deaths in hospitals.”
Currently, hospitals here don’t use compression devices to prevent VTE. The ones back home can cost at a minimum of $4000. The device my team and I spent our spring semester working on should cost somewhere closer to $400.
Inside the PneumaShoe
The PneumaShoe is an intermittent pneumatic compression device that prevents VTE and the formation of blood clots within patients prone to them (post-operative patients and OB/GYN patients). Blood clots, if they break off, can travel to the lungs or brain, where they can block blood flow (as emboli). The blockage of blood flow can be fatal.
During the spring semester, we managed to build a medium-fidelity prototype, a proof concept model which had to be manually controlled during operation. Christine, one of my teammates who came to Malawi for the same internship, and I hoped to learn about automating this process. We wanted to use a microcontroller to run the device through its duty cycle and ideally be able to interact with patient input.
Our solution was the Arduino, a microcontroller capable of running basic programs. In theory, the program should’ve been simple enough to write. In practice, the amount of head-scratching and “Why isn’t this working?” conversations occurred pretty often. It was always the smallest bugs/errors that gave us the most trouble. Eventually, we had the program running an early version of our device’s duty cycle.
Figuring out the hardware wasn’t any simpler. Sifting through datasheets, searching for the right components all took time and patience. Each hiccup, each mistake was another chance for us to learn a little more about circuitry and its nuances. (We learned a lot.)
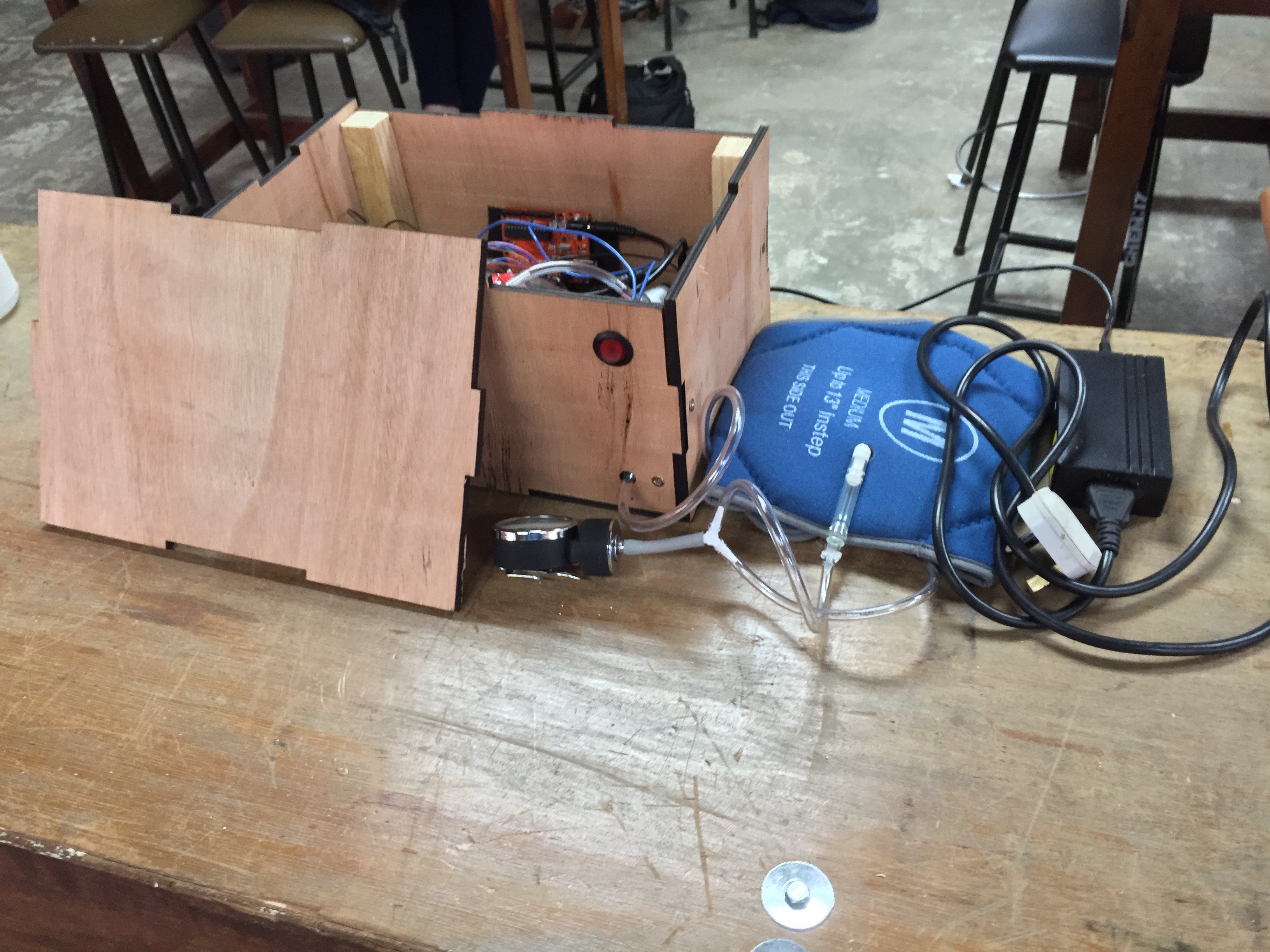
Pneumatic Compression Medium-Fidelity Prototype
Finally, we had our device, all of its components connected by countless wires to one another. Of course, the first thing we did was hide the mess of wires and the Arduino inside of a box. If we were going to present this device, it’d have to look like any other medical device, complete with an on/off switch.
As someone with a tendency to talk, to get excited about the smallest of things, keeping this phrase in mind as I spent my five days walking through the halls of Kamuzu Central Hospital (KCH) played an important role in my data-gathering. A lot of what I did was listen and watch. I talked only to ask questions or to introduce myself to the nurses and patients I came across.
Those first few days I was nervous. Would we able to get enough information? Would the nurses and physicians take the time to speak with us – strangers and students? These questions rattled around inside my mind as we set foot onto KCH’s sprawling campus.
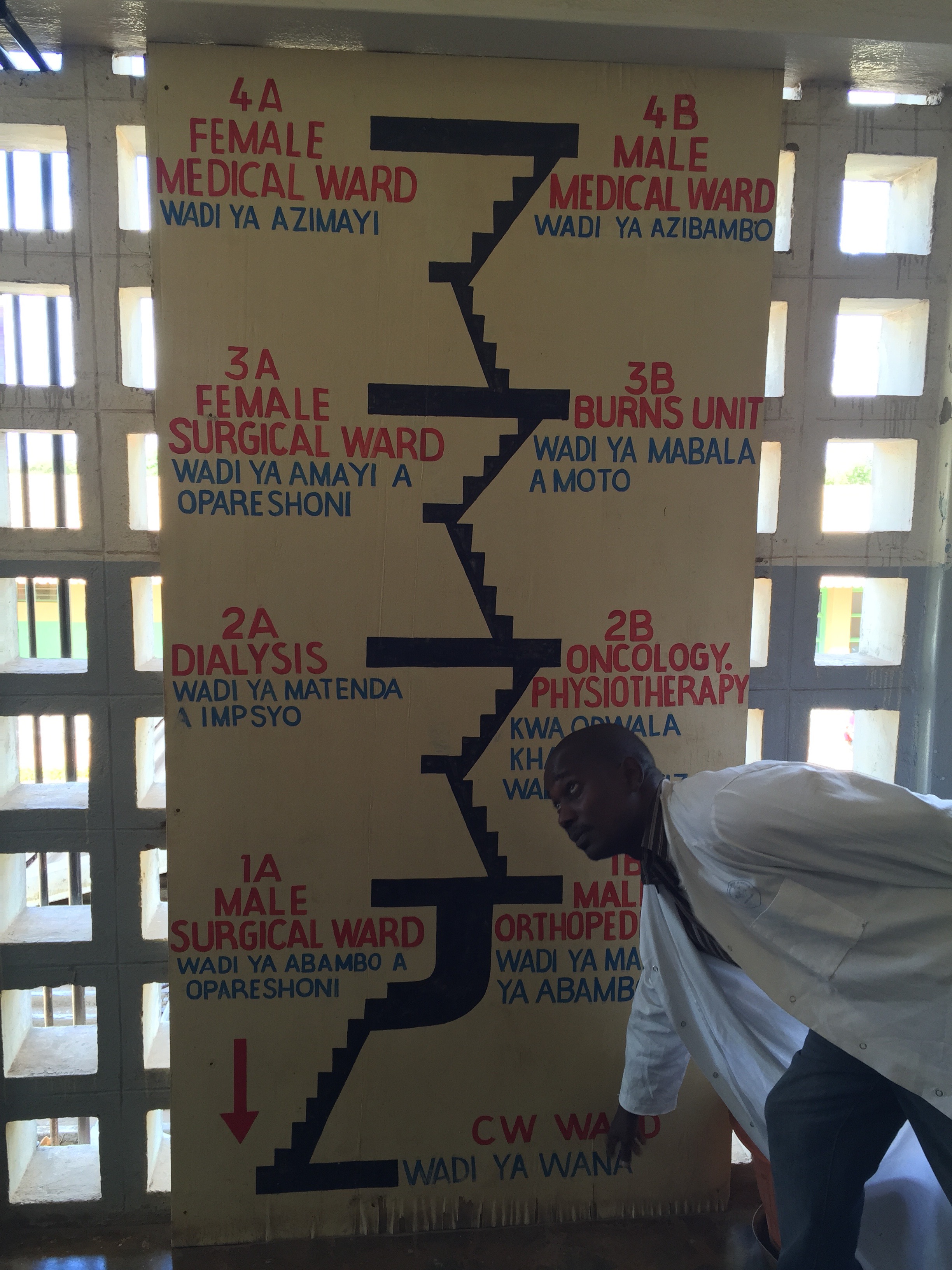
Map of Surgical Wards
On that first day, the tour we were given at the hospital left me feeling more lost than when I first arrived. Before I asked any questions about hypothermia, before I started working on the concentrators, I got lost. I wandered through the hospital with a single purpose: to understand where I was and the people I was working with. It took some time, but eventually, I knew which wards I wanted to visit – the labor ward, the nursery, the kangaroo mother care ward, and the large number of wards with oxygen concentrators ranging from pediatric to surgical wards.
O2 Concentrator in Pediatric Ward
I spent some of my days taking apart oxygen concentrators, documenting their faults, and speaking with the hospital’s Physical Assets Management (PAM) engineers. The rest of the time I spent in the wards. Where I could, I took the time to watch and observe, paying attention to the way the nurses worked, the way patients behaved, and the way the wards were set up.
Along with the observations, I talked with nurses and physicians learning about hypothermia and the concentrators little by little. Each story shed some more light on the challenges we might tackle as students and biomedical engineers.
Over these last 5 days, the physicians, nurses, and engineers I worked with taught me a little bit more about what it means to be an engineer and helped me understand a little better what role I might play in the future as a physician and engineer. Thank you, Kamuzu Central Hospital, for welcoming us with openly and warmly!
I had come to Morning Meeting to learn about hypothermia, and the stories I heard answered some of my questions and gave me new avenues to consider. But what left me captivated was the nature of the meeting itself.
Morning Meeting Conference Room Table
7:55 am. People trickled into the conference room. Slowly, all the seats filled, leaving only standing room. The physicians, 20 or so, sat around the conference table in the center of the room. The rest of us and the medical students sat in chairs set against the 4 walls of the room.
8:00 am. The doctors started speaking.
“A boy was brought in…”
We worked our way through the little boy’s story, learning about his illness prior to his arrival, hearing what happened during his time in the hospital, and his outcome.
“A baby girl was brought in with a fever…”
This was Morning Meeting. Mistakes were laid bare, yet this wasn’t a place for rebuke. It was a place for learning from those mistakes so that the 40 or 50 doctors and medical students in the room wouldn’t repeat them. Whether it’s here in the conference room in Kamuzu Central Hospital or back home on the 3rd floor of Texas Children’s Hospital, there’s a burning question that never goes away.
“Why?”
Why that outcome? Why did that patient present in that way? Was there something else that could have been done? Morbidity and Mortality conferences, M&M’s, are a reminder that in the world of medicine, we’re constantly students. Our operating rooms, our patients, our colleagues are all our teachers.
I wince as I turn the oxygen concentrator on. A shrill alarm fills the air, informing me that the concentrator’s powered up, and a loud hum fills the air as the compressor inside starts to suck in air.
I’m taking apart an oxygen concentrator in Lilongwe, Malawi’s Kumuzu Central Hospital. Next to me, Harvey, my partner from Malawi’s Polytechnic University, jots down an oxygen concentration as I hold the concentration meter’s tube close to the concentrator’s nozzle. We don’t have an adaptor, so I’m holding it steady as best I can.
“Is this thing o -”
The numbers start to jump. 22, 34, 56, 63.
Grimacing, I look up at Harvey.
“Concentration’s at 63%. It should be hitting 90%, at the least.”
Our first day in Kamuzu Central Hospital marks the start of a 5-day pursuit. Our goal here is two-fold. First, we’re trying to figure out why so many oxygen concentrators fail.
Queen Elizabeth Central Hospital – Oxygen Concentrators in Need of Repair
When these concentrators break, they’re brought to the Physical Assets Management (PAM) department for repair. The engineers here in the hospitals are filled to the brim with these machines. Instead of being in use, the machines are stranded in the workshop with the PAM engineers doing their best to get them up and running. Even after our first day, seeing the engineers here strip down broken machines for parts and repair concentrators with what they have available has inspiring to see and be part of.
We want to figure out why so many of these concentrators fail. Is it a rogue resistor, burned out due to a power surge? Has the compressor failed? Have the filters gone bad? Are the sieve beds that help concentrate the oxygen faulty? What’s the weak link in the chain? By taking these concentrators apart, by performing diagnostics on them, we are trying gather enough information to start designing long-term solutions to common modes of failure with these concentrators.
Our second goal is to study the “warm chain” for neonates after they’re delivered. Our goal is to reduce the incidence of neonatal hypothermia, and in order for us to do that, we need to understand what happens to neonates once they’ve been delivered.
With both of these goals, we’re talking with nurses and physicians, making observations, and doing our best to paint a full picture of the needs that are present. The work we do during our week here in Lilongwe along with the other clinical sites being visited will form the foundation for the next 5 weeks of our internship. This part, the needs-finding, is a reminder that carefully considering what the problem is just as important as designing the solutions to address the problems.
If we leap too quickly, the solutions we design won’t address the true problem. As a student, we’re often presented with carefully crafted problems and asked to fix them. Rarely are we able to carefully forge a problem on our own. Rarely do we get to scope out the field, compile observations and interviews, and transform that data into a thought out need. But that’s exactly what we’re doing during this week. Let’s see what the bigger picture ends up looking like!