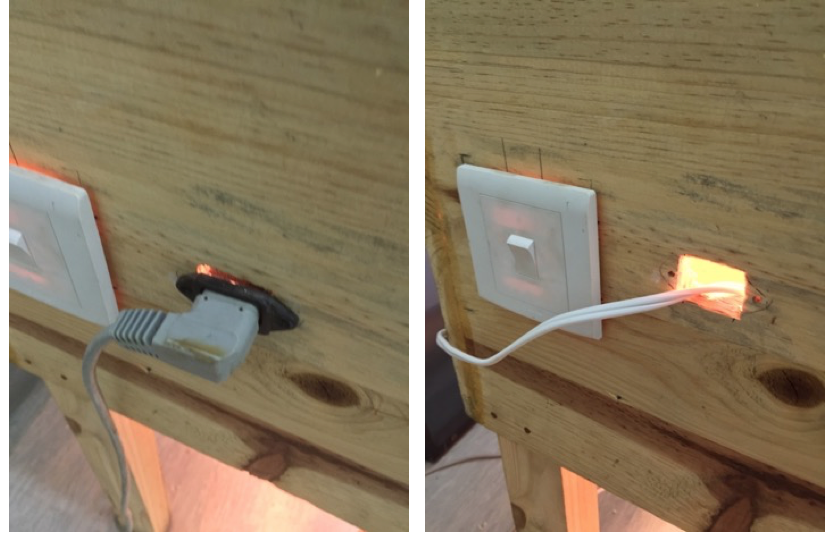
One of the first things we realized with the Chitenje Warmer was that a temporary power cord wasn’t going to work. When we found it the first time around, the device had been missing its power cord, so our solution in this case was pretty straightforward. We made and installed a permanent power cord into the device. This way the device’s functionality wasn’t dependent on an external power cord.
Once we overcame the technical barriers, the next step was to relocate the device so that it could better serve its target population (neonates delivered via c-section). Upon the advice of Dr. Meja, we moved the device to the labor ward operating theaters. Once we got it into the theaters, we had to figure out how to integrate the device into the nurses’, physicians’, and midwives’ workflows.
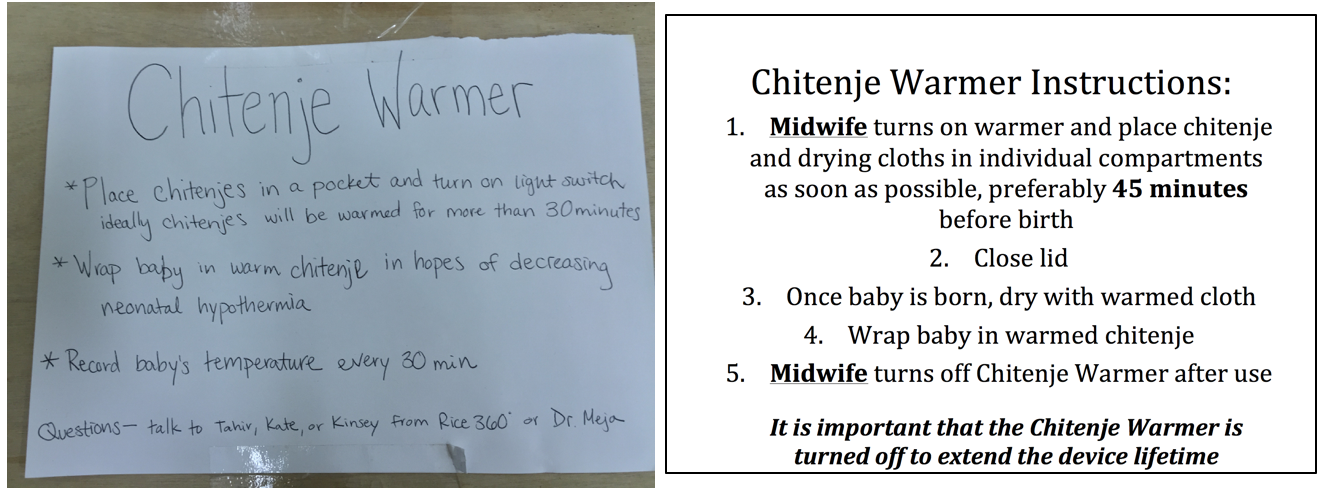
By itself, the device was wooden box with an on/off switch. We needed to add labels and instructions so that the nurses and midwives who’d be using the device had some sense for what it was they were using. We drafted up a set of instructions, and I sat in the breakroom for a bit, showing the instructions we had drafted to a few of the nurses.
“Someone needs to be in charge of the device.”
-Nurse, Labor Ward Operating Theater
After a little while, we had a clear idea of what our instructions needed to look like. For sure, the instructions had to include which set of healthcare provides (the midwives) would be in charge of using the device and turning it off when it wasn’t in use. The passive instructions we wrote were only part of the picture. I also actively oriented nurses and midwives whenever I could in terms of how to use the device.


Active Orientation
Part of this meant waiting in the break room, walking with nurses to where the device was being used, and asking if they had seen it before. A fair amount of the time I would find the midwife before the c-section was started and ask them if they had seen the device yet.
Overcoming the technical challenges, designing a set of passive instructions, and orienting nurses and midwives was a part of the design process I hadn’t seen before. As a student engineer, I’ve often gotten to the prototyping stage, but this was the first time I was working to implement a device inside the hospital. It’s hard to appreciate the nuances involved with human factors until you’re actually trying to get a device up and going in its intended setting. Even now, there’s still so much to do, but we’re getting there little by little!