Time has a weird way of passing once you build up a routine. At first each day seems like an ordeal, a deep underwater dive into a new world where a day is only marked by new discoveries, not hours. Then when you break the surface and look back, what seemed like a week has somehow turned into two months. That’s only a fraction of the wonder I’m feeling at how we have adjusted to life here. While I had some expectations coming into the summer, I think it’s a given that life will throw whatever it wants at you and you just pick up the lessons along the way. So in the spirit of learning, I wanted to share some of the things I did not expect to do/learn during this summer.
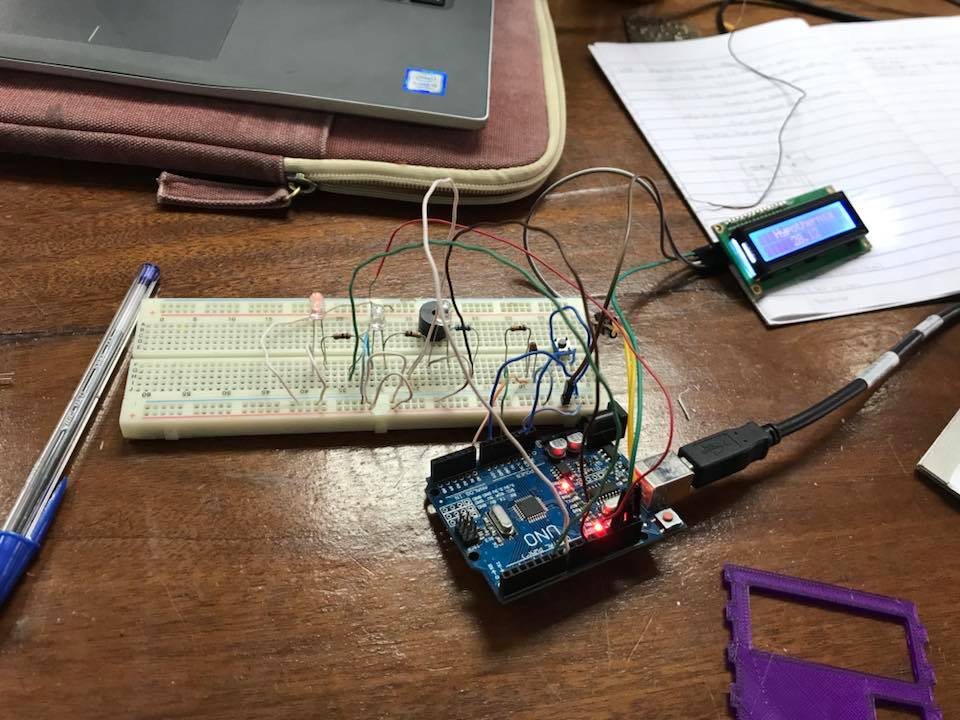
- Coaxing a 3D printer: The first time I 3D printed something was during the internship training at Rice’s OEDK. Even though it was tricky trying to squeeze in your project among the others, the printing process was smooth sailing. At the design studio, they have a Prusa machine that gets quite finicky in the cold. The plastic sometimes drags and I have to watch the machine like a hawk (positive reinforcement also helps). But at the end of the day, I’ve learned so much more about the process of 3D printing and using CAD software like Solidworks.
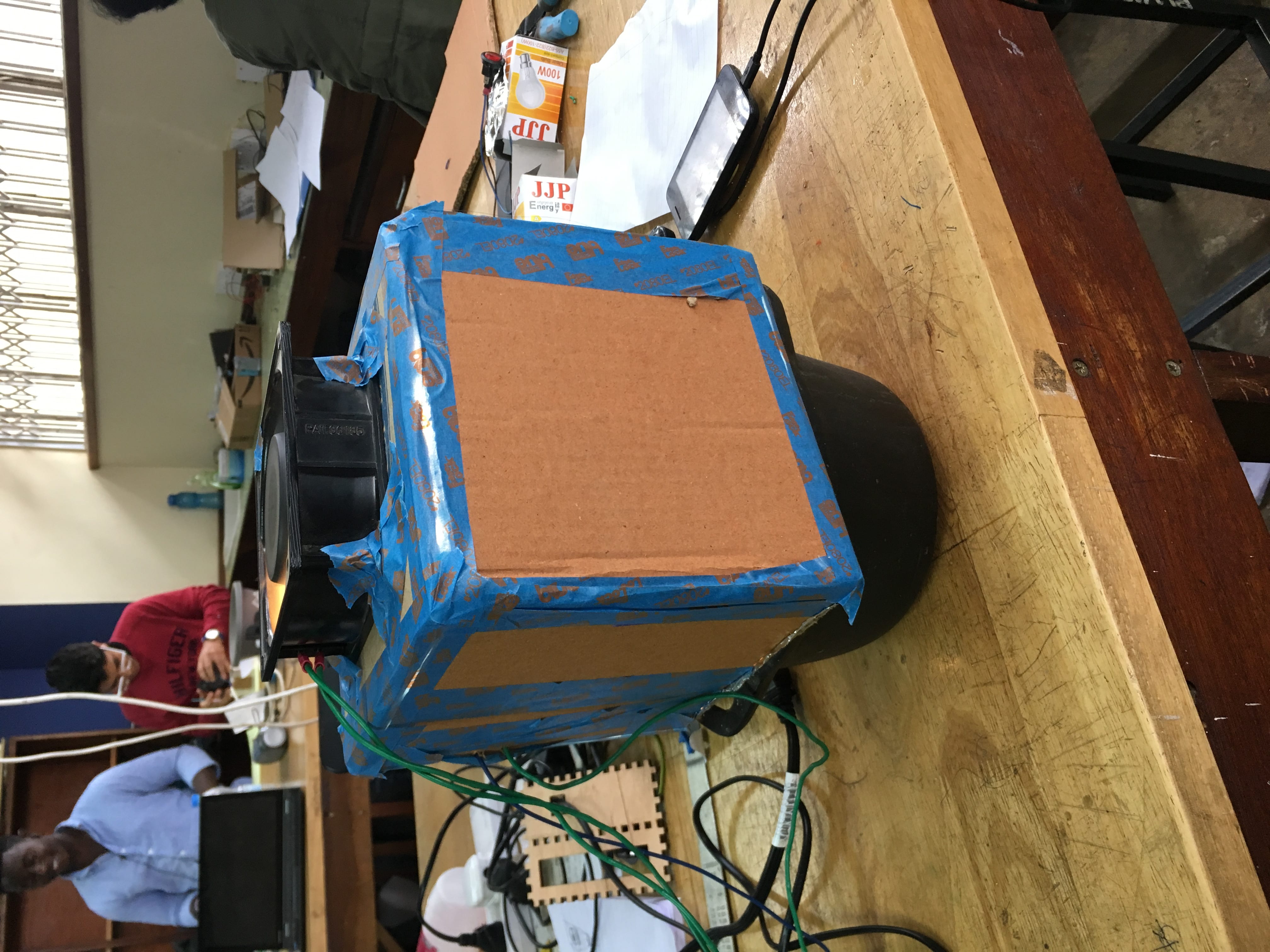
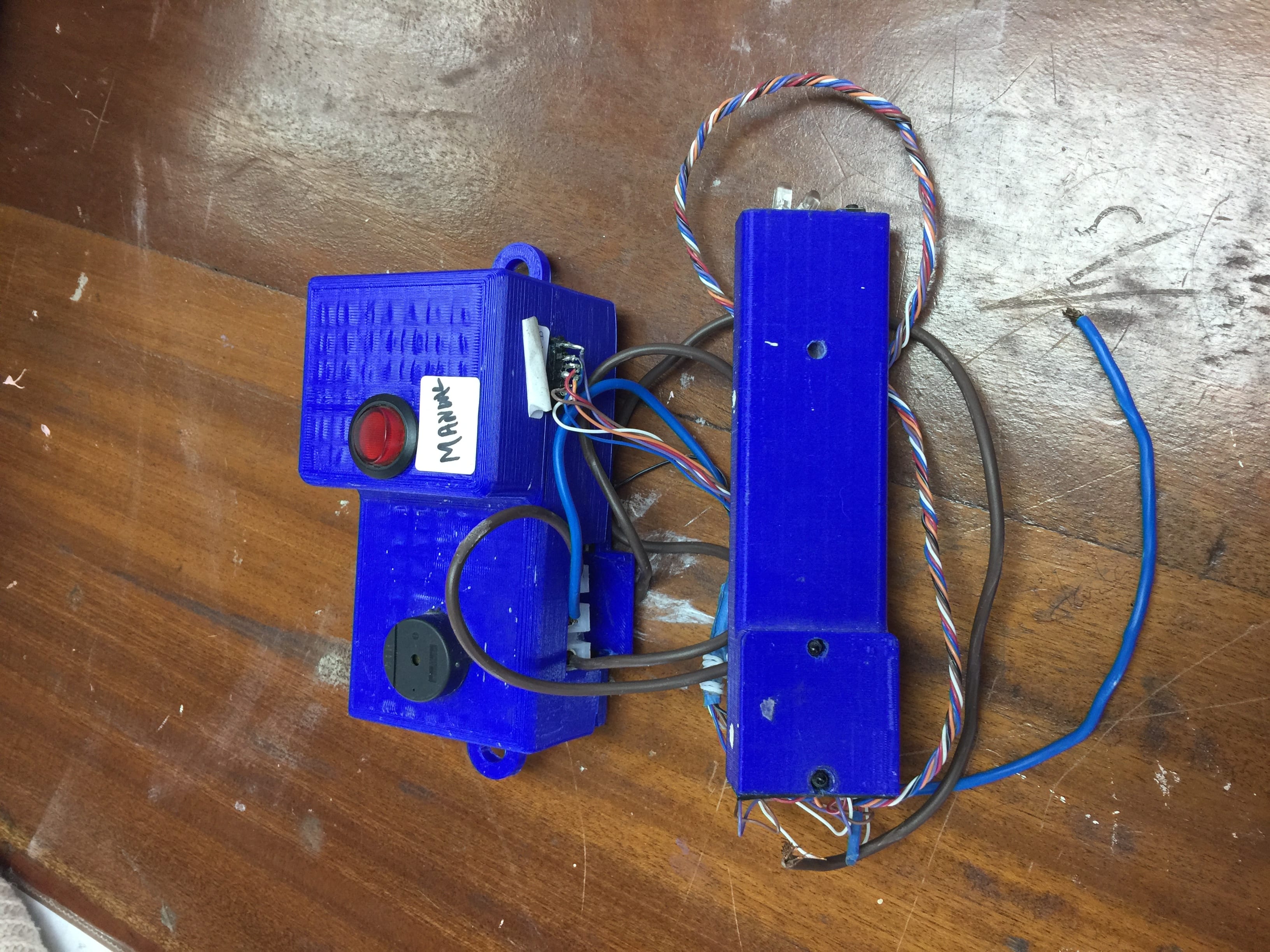
- Making an oven: Alright, maybe it can’t be strictly classified as an “oven” but our device is resembling more and more like one everyday. In our original quest to regenerate zeolite, we found that the industry standard is to pass hot gas/air over the molecular sieves. Past teams have also used an oven to dry out the zeolite externally. While we want to push hot air through the sieve bed canisters, in the process of doing so we’ve researched a lot into household heating appliances, namely the oven. While it’s not quite at the final stage, the purpose of the box is to insulate the heat produced by the light bulbs inside, thereby warming the air above it.
- Teamwork makes the dream work: The hidden clause in being an engineering major is that you get used to working in a team for everything. Problems are no longer straightforward. Every new mind that looks at the problem is a new approach that could lead to a better solution. Communication styles differ here in Malawi compared to the States. People tend to be more indirect and lean on the more polite side. It definitely took some getting used to and our project was confused in its direction in the beginning. I feel like this has been a good practice at being a better listener and observer.