Next week we will be travelling to other hospitals in pairs. I am travelling with Kate to Zomba, where we will perform oxygen concentrator tests and observe a few wards.
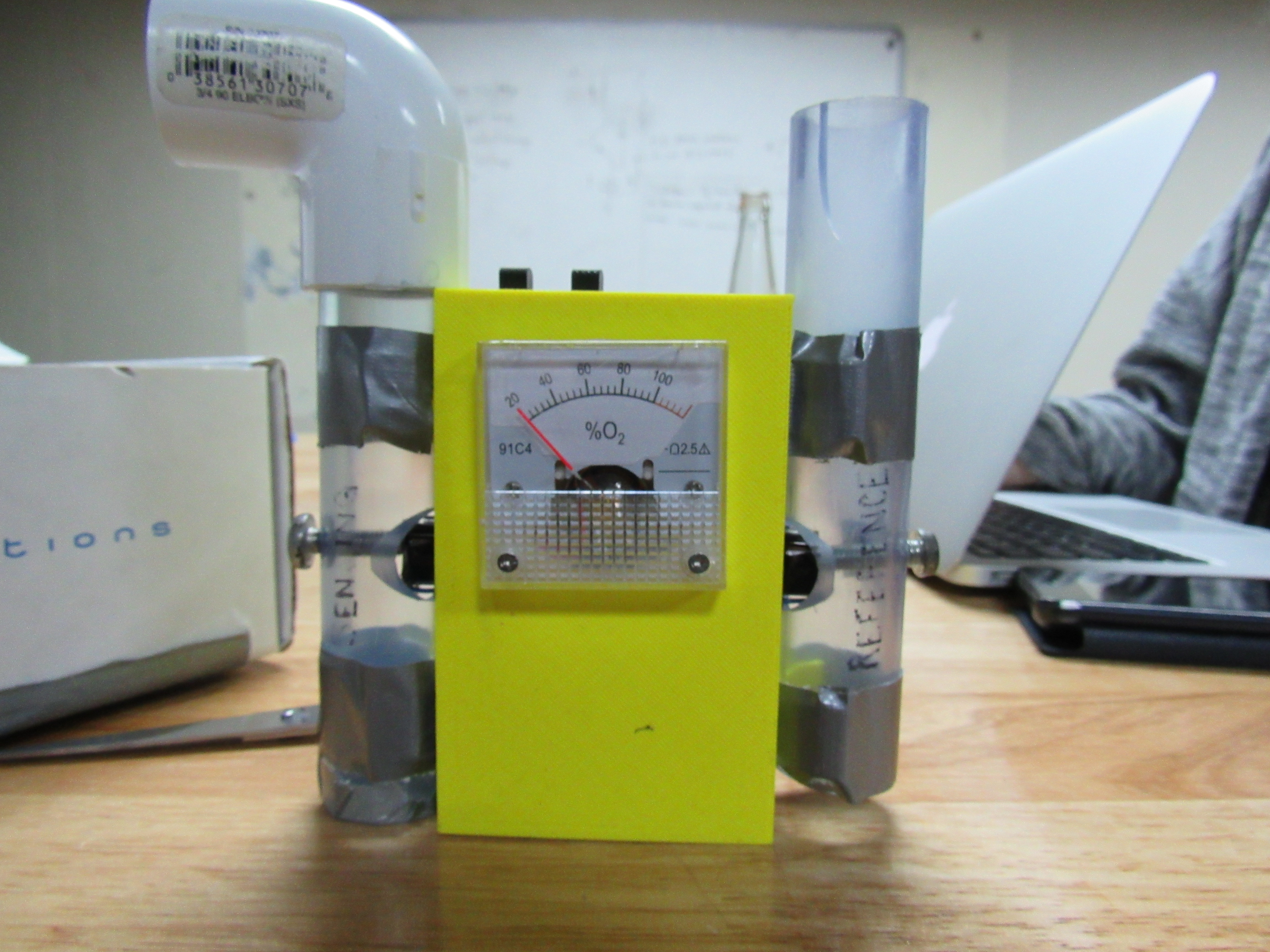
This past week, we have been extensively studying the components and operation of oxygen concentrators. We have read through user manuals, taken measurements on some broken concentrators that are in the design studio, and opened them up to analyze their parts. In preparation for our trips, we have created a data log to record the oxygen concentrations and flows being outputted by the machines we encounter, among other measurements. One of the four toolkits we created for each team is pictured below.

Oxygen sensor, pressure gauge, flow meter, DMM, tubing, screwdrivers, etc.
While we have learned a lot about repairs, we will be working alongside the PAM (Physical Asset Management) technicians, who maintain medical devices in Malawian government hospitals, to do any repairs (not performing them ourselves). Independently, we will be working on diagnosing the issues we find and creating a detailed database so that when we return to the Poly, we can determine common issues occurring as well as their frequency, and perhaps find some non-traditional solutions. We want to especially focus on making them easier to repair locally, because having to order parts is not ideal in this setting. Of course, in addition to any suggestions we make, Matthew Petney has asked us for a detailed risk assessment, as we will be proposing alternatives to standard repair methods.
Our observations in the wards are focused on the treatment of neonatal hypothermia. Hypothermia in neonates is a known issue in low-resource settings, but lacks research and low-cost solutions. While several devices have been designed to aid in the thermoregulation of neonates in low resource settings, not many studies exist comparing the effectiveness of each one.
Preventing hypothermia boils down to the methods of heat transfer: conduction, convection, and radiation. Within each of these categories lies a plethora of minute details which must be accounted for to prevent heat loss. For example, if a newborn is placed on a scale for a few minutes after delivery while the mother is still being cared for, any contact with the cold metal of the scale will draw heat from the baby. Any draft in the room as well as washing the baby too soon after birth facilitates heat loss through convection. Drying and swaddling is a standard method for hypothermia prevention, but this is much less effective if the baby is swaddled in the same cloth that was used to dry (common if only one cloth is available).
We will pay close attention to every detail of the babies’ setting: proximity to open doors or windows, ambient temperature of the room, etc. Behavioral factors like temperature measurement methods are also important. We visited the neonatal ward in Queen Elizabeth Central Hospital today, where we noticed that only one nurse was on duty in a large room full of neonates. Most care was provided by mothers. We spoke to a few, who said that they measured their baby’s temperatures with the backs of their hands, a common method where thermometers are not available to every mother. We are hoping to shadow a nurse in the ward, speak to some mothers, and maybe even observe a delivery to better understand common thermoregulation practices.