Hello everyone!
It has been such a whirlwind of a week (2 weeks?) since I wrote my last blog entry. I have many new updates to share so I’m just going to dive right in.
This past week and a half, Liseth and I have been busy continuing our usability observation project. We wrapped up our note taking from Queen Elizabeth Hospital with a visit to the pediatric oncology ward, pediatric special care ward, and an overnight stay in the neonatal intensive care unit (NICU). From speaking with nurses in oncology, we learned that the lack of syringe infusion pumps meant that nurses had to calculate the average amount of fluids and chemotherapy drugs administered per hour. They discussed with us the challenges of manually regulating these dosages for every chemotherapy patient.
While spending the morning in the special care ward, we observed that the bulk of the medical equipment and technologies (oxygen concentrations, bCPAP machines, patient monitors) were concentrated to the high dependency unit (HDU) for special care patients requiring respiratory support. At first, we were surprised to see that all of the patients were in the HDU and the main bay area beds were completely empty. But around 9am, floods of kids and families entered the ward from outside and filled up almost every bed in the main bay area. In the special care ward, patients and their families must gather their belongings and leave their beds to wait outside twice a day while the ward gets cleaned in the morning and afternoon. We learned that many of these main bay patients were typically kids suffering from anemia, malaria, HIV, and tuberculosis. These serious conditions would generally warrant the use medical equipment and monitoring devices, however the limited resources available simply must be used towards the HDU patients.

Our overnight stay in the NICU at Queen Elizabeth was my first experience spending the night in a hospital setting. I did not really know what to expect, as my hospital expertise stems from episodes of Grey’s Anatomy. At Queens, we noticed that the night shift was when many of the babies get put on and taken off of different medical devices. We saw the setup of oxygen concentrator machines, the preparation for phototherapy treatment, and the administration of various drugs. The night provided excellent insight into how nurses and doctors interact with the technologies and Liseth and I got pages of informational notes from our time here.
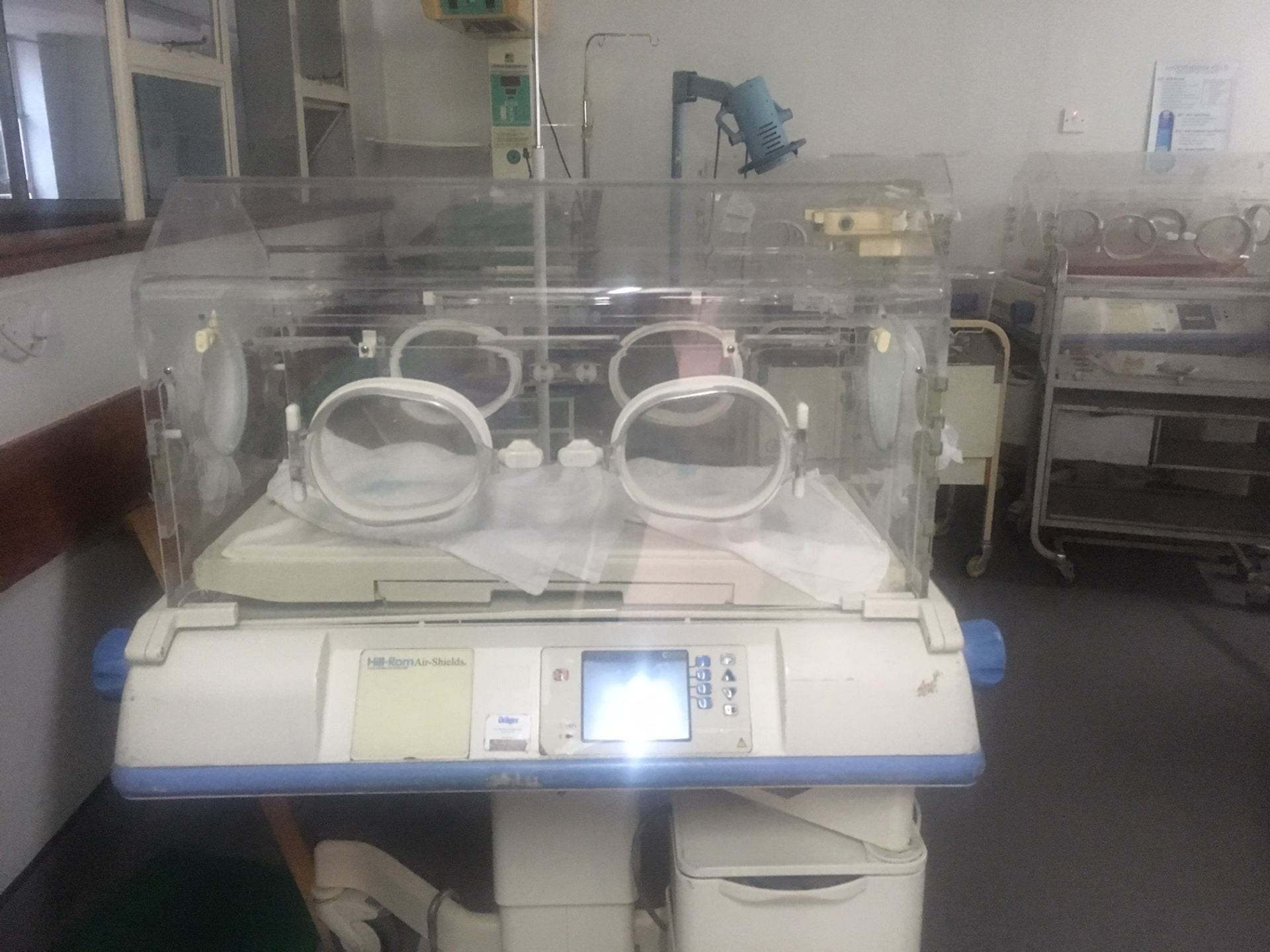
Our next overnight visits provided additional insight into the night routine and ward procedures for Zomba Central Hospital and Mulanje District Hospital. The Zomba Central Hospital nursery was quite large; it had 4 separate rooms for high risk patients, low risk patients, patients who were brought in from home, and for kangaroo mother care. 1 continuous monitor was available for all patients to check vital signs so again, Liseth and I watched as a lack of resources continued to influence healthcare and outcomes. Seeing the nurses face difficulties to keep neonates alive was extremely difficult and probably the hardest part of my internship experience so far. Our overnight visit at Mulanje shared many similarities. Here, human resources were scarce as 1 nurse was on the night shift for the entire ![]() NICU. No continuous monitor was available for the ward, so vital signs and recording were limited to temperature checks using 1 thermometer for all the neonates.
NICU. No continuous monitor was available for the ward, so vital signs and recording were limited to temperature checks using 1 thermometer for all the neonates.

The health inequalities were extremely evident as my mind couldn’t help but draw comparisons to the equipment availability in the United States. After looking more into a holistic economic picture of the country, I learned that Malawi suffers from a climate vulnerability that has widespread influence upon agriculture, energy, forestry, water, gender issues, and human health. In 2015 and 2016, Malawi suffered from a pattern of floods and droughts that impacted over 5 million Malawians with food insecurity. Any extreme floods and droughts of a growing season can be detrimental to the climate-sensitive agriculture sector which contributes to up to 40% of the gross domestic product, employs 85% of the workforce, and supplies 70% of raw materials for manufacturing. With an under-financed health sector, 60% of the country’s total health expenditure needs to be obtained from external sources such as donations. Reports suggest that in order to break out of a cycle of systematic poverty and dependency, Malawi needs to target the rural poor who depend on mainly agriculture alone for subsistence. Expanding the access and quality of health services available these rural communities in Malawi would help address some of the social, economic, and environmental determinants of health as a means of reducing overall health inequities. (Based on WHO Country Cooperation Strategy: Malawi https://apps.who.int/iris/bitstream/handle/10665/136059/ccs_mwi.pdf;jsessionid=55B8169FD0E2EFBE8B253B154BF5AF96?sequence=3).
When examining global health, I feel that it is incredibly crucial to consider all influences and factors that contribute to current health situations. Policy reforms targeting healthcare delivery and accessibility systems, human and monetary resource allocation, and overall health development are so vital to helping alleviate morality and disease burdens for a country. Although it can be an uphill battle, tackling global health with a comprehensive economic and policy approach lays the groundwork for sustainable widespread change.




Thanks for reading! I’ll check in again soon for my last week in Malawi! See you next week!