Day 7
We split our group up into two teams and ventured to some district hospitals today (we always move in a pack so this was the first time we separated). We planned to focus our visits on three aspects of the hospitals: the nursery, maternity ward, and PAM (physical assets maintenance area or the place where hospital staff send off broken medical equipment). Prince, Andrew, and Jeremy (a bioengineering student) first took me and Sajel to Mulanje. I thought Queens was different, but the Mulanje district hospital wasn’t like anything I’ve ever seen.
The hospital in Mulanje was about an hour and a half drive from Blantyre. We drove up a winding hill and reached the hospital, which was at the base of Mount Mulanje. The clouds were so close I thought I could touch them. The hospital was much smaller in size compared to Queens because Mulanje is a district hospital. Prince explained to us that there are three levels of medical care people can receive. People will first go to small local health centers, which are spread throughout all districts in Malawi. The health centers have midwife technicians and medical assistants, but no clinicians or doctors. If the condition is too severe, people can be referred to the next level of care at district hospitals. They are larger and have one clinician, a registered nurse at every ward, and interns. These district hospitals are better equipped at handling more serious conditions, but may not have specialists or general surgeons. As a result, people may then be referred to the final level of care at central hospitals (such as Queens). Prince told us that it is important that the earlier levels of care are improved as this will reduce the amount of time people have to spend untreated. If people have to be constantly referred, they will spend more time travelling to far off hospitals and risk making the condition more serious.

Our first stop was the nursery. We walked into a small room with cots lining the walls. The registered nurse greeted us before we asked her some questions about the infant ward. We talked A LOT, but I’ll only cover a few of the things we discussed:
- The registered nurse told us that power outages were extremely common. Although they do have backup power via solar energy, this only lasts about an hour before running out. Babies with hypothermia who are placed under the radiant heaters are at risk and must be put in Kangaroo care (warmed by their mothers’ body heat). As a result, hypothermia is a leading cause of infant mortality at Mulanje
- Birth asphyxia is another primary cause of infant death at Mulanje because there are no available oxygen concentrators.
- Gastroscesis (a condition where babies are born with their intestines outside of their body because of a large opening at their stomachs) is very common. But these babies are sent to the central hospital. Plastic gastroscesis bags to hold and protect the intestines are not available, so the babies intestines are covered with gauze as the baby is transported to Queens. This is very dangerous, however, because the gauze absorbs moisture from the intestines, destroying them. Sajel showed her prototype gastroscesis bag to the nurse and she got some great feedback!

After thanking the nurse at the infant ward, we moved on to the labor ward. It was very busy when we visited, so we couldn’t spend very much time there. It was so crowded, in fact, that all the beds were taken and patients had to be treated on the floors.
- Thermometers are not available (because they break down or are missing), so nurses have to check the temperature of mothers using their hands. Fever is extremely common because of malaria births, so lack of thermometers is a huge problem (I was also able to briefly show them my prototype and the feedback I got was extremely helpful!)
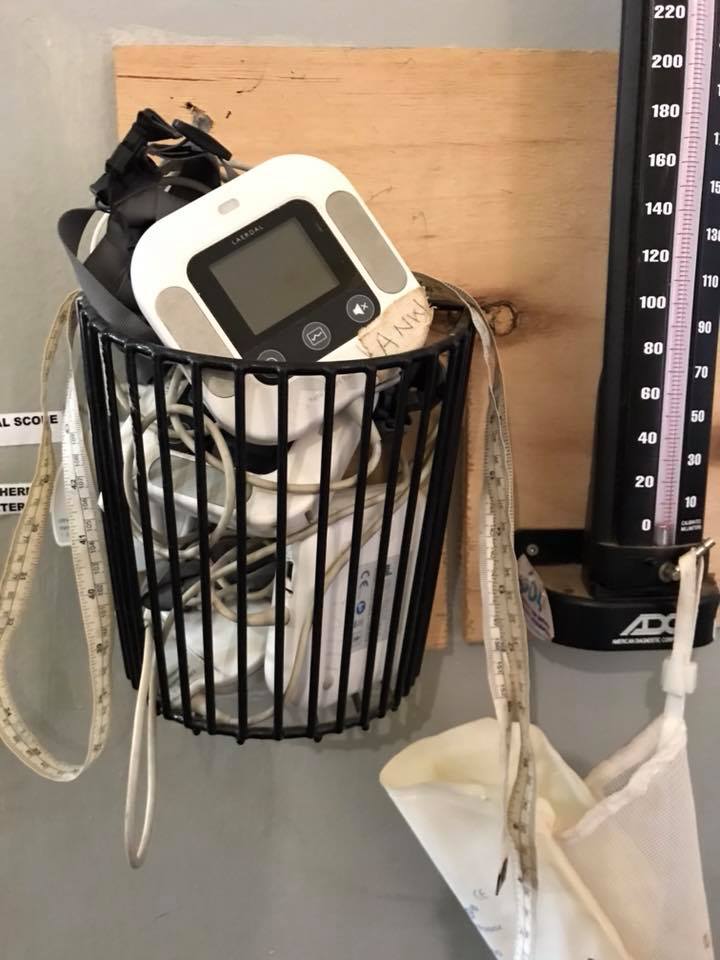
- The nurses use the metal fetal heart beat scopes to check the status of the fetus during labor. There are only a couple and with over 30 patients being seen every 24 hrs, it can be difficult to constantly monitor the fetus. I looked behind me and noticed a box of 4 or 5 fetal monitors and I asked why they weren’t used. The registered nurse told me none of them were working and that no proper training was given when the devices were introduced at the ward. Prince told us that checking the fetus is crucial because if they notice something wrong, they can take immediate measures. But without knowing how the fetus is doing, labor may be prolonged. As a result, birth asphyxia is a common condition there.
We drove another hour and went to the much larger, much newer Thyolo district hospital. Thyolo sees almost double the number of patients as Mulanje, but there are almost the same number of nurses still on duty. As a result, constant monitoring for the patients is quite difficult. There is a high rate of birth asphyxias as a result of fetal distress during labor (due to the inability to continuously check the status of the fetus). Gastroscesis is also a common condition seen by the nurses, occurring about once every month.
What stood out to me most on our visit to Thyolo was something the registered nurse at the infant ward told us. She said that the members of the CPAP team for Rice 360 were their only suppliers for supplies like oral gastric tubes and suctioning tubes. If the CPAP team were to stop visiting the hospital, Thyolo would lack a sustainable supplier for these medical equipment. This was really shocking to me because without these devices, it is very difficult to provide oxygen for babies with birth asphyxia and nutrition for premature babies who lack the correct reflexes to feed.