Last week was full of travel! On Wednesday, we had the opportunity to head to Lilongwe for the annual CPAP Coordinator Peer Review Meeting where each of the twenty-eight hospital coordinators come together to present their hospital’s previous year of data collection, CPAP successes and challenges, and action plans for the coming year. This meeting was a great chance for us to see yet another side of program planning and implementation: How can we assess success and failure in a way that leads to progress and sustainable planning for the future use of CPAP in Malawi?
We were able to see a lot of motivated coordinators, but the major challenges that each of them face will require hard work in the coming year. Despite regular trainings for hospital staff, CPAP coordinators struggle to keep trained nurses in the maternity and neonatal wards due to frequent staff rotations by management. A lack of trained staff on the wards then leads to a lack of confidence in putting patients on CPAP, so patients put on CPAP steadily decline as trained nurses rotate out. Keeping trained staff available requires strong advocacy and lobbying by hospital coordinators as they work with management to prioritize improving neonatal care.
Several hospitals also struggled to collect ample amounts of data due to already short-staffed nurseries, and the 4-hour monitoring requirements for patients on CPAP increase workload on the already overwhelmed nurses. In some cases, hospital coordinators reported having as many as 70 babies in a nursery staffed by just a single nurse. In a project where data is one of the most powerful tools for proving CPAP’s effectiveness, it becomes critical to understand the barriers to collecting and recording that data. In this sense, the meeting was incredibly helpful, as it allowed a forum for coordinators to come together to see how other districts were performing, which data collection strategies were showing success, and discuss ideas for further improvement. The exchange of ideas and enthusiasm was exciting to watch as each hospital drafted an action plan for the next three months at the end of the meeting.
The peer-review style of discussion was a great way to increase both enthusiasm and accountability for each hospital coordinator. By presenting his or her hospital’s progress to the group, each coordinator was able to critically evaluate his or her work and identify areas of success as well as areas of improvement. There were also nine coordinators from Phase III hospitals in attendance, and Phase III hospitals are gearing up for CPAP installation in August. This meeting gave them a chance to learn from their Phase I and Phase II colleagues on how to mitigate challenges from the outset, and the meeting fostered discussion between these newer CPAP hospitals and hospitals that have been operating with CPAP for some time now. The energy from the Phase III coordinators also added a unique element to the meeting, and it will be exciting to see how their implementation plans move forward in August upon installation!
Spotty access to wifi has actually turned into one of the best things about our time at home in the evenings. It’s given all of us more time to reflect on and discuss our experiences from the day, and we’re also able to get tons of great reading in. One of the books we’ve been passing around is The Bright Continent: Breaking Rules and Making Change in Modern Africa by Dayo Olopade, and it has given me an entirely new insight into how countries in Africa have been creating innovative market opportunities and economic growth in recent decades. It also delves into the dynamics of aid-based economics and the way that this approach can often be detrimental to the homegrown businesses and markets that are already in place.
One of Olopade’s main focuses in the book comes from the concept of kanju, the creative solutions that are common in resource-limited settings across many African countries. Tanya wrote a great blog on the kanju and several of the examples we’ve already seen of it here at Queens and in Blantyre, so definitely check out her post here to get a better idea of it!
The most interesting example I’ve seen of kanju, however, was during the maternal mortality meeting that I also spoke about in my last post. Hypothermia is always a huge concern for infants, and in delivery conditions that are not thermally regulated, helping babies maintain body temperature is a challenge that begins immediately after birth. While a technology design could theoretically fill this need, the amount of time that it would take to move from design through testing and development could span any number of years. In the meantime, however, babies still need help thermoregulating, and doctors and nurses are continually looking for interim solutions. A 2012 study at a South African hospital showed significantly improved outcomes for babies swaddled in a plastic bag after birth, and these babies had reduced incidence of complications from hypothermia. A single plastic bag at a grocery store costs 35MKW on average (~0.09 USD), and in bulk, that cost would likely shrink even further. The bags are an example of a readily available, low-cost resource that clinicians and nurses at Queens are able to use without having to wait for a technology to fill the existing gap.
This is just one example of how the hospital staff continually identifies creative, practical solutions to the challenges they face every day, and I’m interested to see how they begin to implement the idea in the delivery suite here and track its progress before next month’s meeting.
Once a month, clinicians from Pediatrics and Maternity come together to discuss both specific cases and general coordinated care between the two wards. Maternal and child health are intricately linked, and the more communication and collaboration that occurs between these two departments, the better the outcomes for both mother and child. Tanya, Sarah and I were able to attend this monthly maternal mortality meeting, and one of the central discussions involved making the decision whether or not to induce labor in high risk pregnancies.
Worldwide, rates of cesarean section births usually hover around 15%. However, at Queens, 29% of births were performed by C-section in 2014. This unusually high rate of C-section births points to two major concerns that guided the discussion – first, why are so many C-sections necessary at Queens, and second, how does this influx impact long-term maternal and child outcomes here?
On any given day, the delivery suite at Queens ebbs and flows between the calm of just two or three mothers in labor to the chaos of sixteen or seventeen (more than half of whom are likely high-risk deliveries). Especially for pre-eclamptics or younger mothers whose hips have not developed fully, C-sections offer immediate intervention when fetal distress puts both mother and baby at risk. Queens sees incredibly high numbers of these types of cases, and one theory that came up during the meeting was the fact that prenatal care in district health clinics rarely provides adequate preventative monitoring for mothers due to both personnel and equipment constraints. Oftentimes, expectant mothers don’t seek prenatal care due to the time it takes to travel to the clinic and wait to be seen- a significant economic productivity drain for a population that can hardly afford it. This lack of prenatal preventative care could therefore be a major cause of high numbers of deliveries requiring C-section interventions at Queens.
As for the second question, it’s difficult to tell how significant of an impact that these interventions have on maternal and child health outcomes due to a lack of long-term data on the topic at Queens. Surgical operations alone increase risk of infection and sepsis for the mother as she heals post-operatively at the hospital and in the following weeks at home. As mothers recover from the procedure, any complications she experiences can make kangaroo mother care (helping with infant thermoregulation) or breastfeeding difficult. So from birth, babies born by C-section are already potentially at a disadvantage.
But perhaps one of the most interesting threads of conversation on the topic came from the decision on whether to induce labor, perform a C-section, or postpone intervention. At this point, several of the expatriate physicians brought up the fact that the mother rarely, if ever, actually gets to participate in this discussion. Growing up in the American healthcare system, I’ve experienced physician-patient interaction where information exchange and patient agency in decision making are held as central components of treatment plans; however, in what I’ve observed, the doctor-patient relationship at Queens takes on a different focus. Patients almost always default to the physician’s first decision on all treatment plans without requesting that doctors take the time to explain and discuss different options. This difference has been a striking example of how medicine is rarely as culturally neutral as it appears, and the debate on whether patient preference should factor into clinical decisions shows how the exchange of ideas and standards from expatriate doctors has influenced Malawian physicians’ opinions on what the practice of medicine should look like.
For me, informing patients on the risks and benefits of various options and providing patients with a choice seems like the natural course, but this discussion also helped me recognize that my opinion is very much a result of the healthcare system in which I’ve been raised. For a Malawian mother in labor, her preferences for her doctor-patient relationship could be drastically different. For someone used to a system where physicians make most treatment decisions with little patient input, a sudden discussion about her options could indicate to her that the doctor doesn’t feel confident in making a choice; it would be foolish of me to assume that she would want the same experience as me without involving her in the conversation. So while I think that the idea of patient agency in decision making sounds like an exciting discussion for physicians to be having, it also points me back to the importance of conversations with the patients themselves when shifting the concept of the ideal doctor-patient relationship. Regardless of technological advances or cultural exchange of ideas, medicine at its core will always focus on treating and healing the patient, and patient-centered care requires a careful understanding of the specific patient population itself to best treat and heal.
I had very little idea of what Queens would look like before this internship began. Actually, it’s more that I had a very incorrect idea. I had pored through past interns’ blogs to find what few pictures of QECH they had posted, but what I saw (zoomed-out pictures of the main building at Queens) in no way prepared me for the sprawling expanse of the hospital and its wards. It would be a herculean task to photograph all of QECH, so I settled for photographing one ward: the Delivery Suite.
The first thing you see upon entering the grounds of Queens is the main Accidents and Emergencies (A&E) building, which is the emergency room for adult patients [1]. However, let’s say you’re an expecting mother going into labour. In your case, you would probably head directly to the Maternity Ward [2]. Walking through the halls of the hospital [3], you would go through swinging double doors and into the Delivery Suite [4].
1. The Main Building
2. The Maternity Ward
3. Hallways in the Ward
4. The Delivery Suite
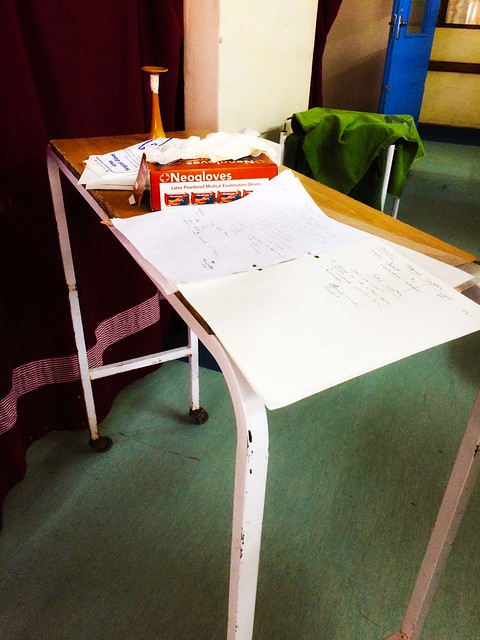
Once in the ward, you would be admitted to one of the bays [5] on either the non-paying or paying side. If your condition were shaky, you would be placed in a bay on the blue high-risk side of the ward [6]. Your charts would be put together, including your admission information and health passport. These charts would then be placed by your bay [7] (or in one of the new holders that Karen and I recently installed in the ward [8]).
5. Patient Bay
6. High Risk Bay
7. Medical Charts
8. New Chart Holders!
In the event that you were having complications or needed additional care, the tireless nurses would come out from their nurses station [9] to attend to you. Running back and forth between the bay and the stocks of medical supplies [10], the nurses would administer any necessary drugs and dispose of their used supplies in the strategically placed buckets in the ward [11]. They would then wash their hands in the sinks inside the patient bays [12].
9. The Nurses’ Station
10. Medical Supplies
11. Disposal Buckets
12. Sink in Patient Bay
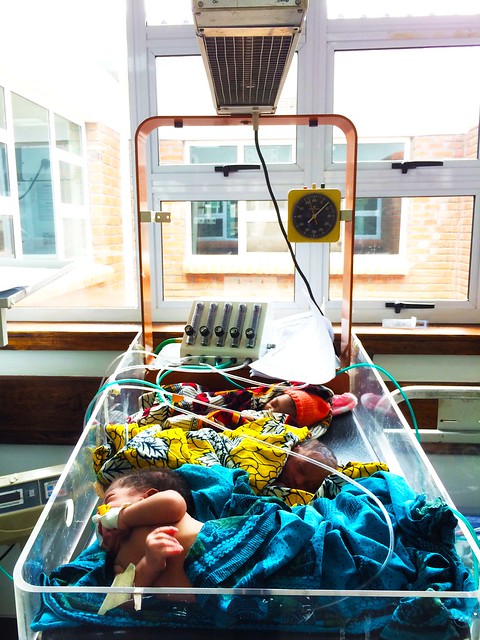
Once you deliver your baby either in the ward or via C-Section in the operating theatre (we can skip the gritty details), your baby may be placed under the radiant warmer to ward off hypothermia while the nurses care for you [13]. The baby would then be delivered to Chatinkha nursery and placed on CPAP, supplemental oxygen, or in a heater as the situation demands [14]. The sheets and blankets would be washed and dried in preparation for the next patient [15], and your delivery would be recorded on the tracking board [16].
13. The Radiant Warmer
14. Babies in Chatinkha Nursery
15. The Laundry Room
16. The Statistics Board
Every day at Queens, this process is repeated numerous times. At one point when we were in the Delivery Suite, 5 mothers were scheduled for C-Sections while another 3 were going into labour within the span of one hour. Moreover, all 8 of these mothers were pre-eclamptic. The caseload is enormous and complex, but the staff at QECH do an incredible job of handling these cases, and they are constantly looking for ways to reduce both maternal and neonatal mortality.
Last Thursday I had the great honor to visit Jacaranda School for Orphans . The other interns and I were invited to come and speak to the students about the various BTB technologies we had brought/made and what we are doing in Blantyre this summer. When the visit was first pitched to us, I’ll be honest and admit I wasn’t too fond of the idea. It would require us taking a morning off of work to go talk to a bunch of rowdy kids who probably wouldn’t understand or care about what we had to say. I freely and happily admit my preconceptions couldn’t have been more wrong.
Almost immediately after disembarking the taxi, we were graciously greeted by the school director and two bubbly students – Alinafe and Jarrod – who would serve as our tour guides. The dynamic duo walked us all around the campus’s pristinely manicured gardens and brightly painted buildings. We walked into several classrooms, and without fail, were greeted with a standing ovation and a dozen or more smiling faces.
One of the buildings with murals of book covers.One of the student gardens.
After our tour of the facilities – including classrooms, a library, a clinic, a computer lab, a small barn, and an arts and crafts garage – we were taken to a large room where all of the students had been assembled. There was a buzz of excitement in the air.
Jacaranda assembly room
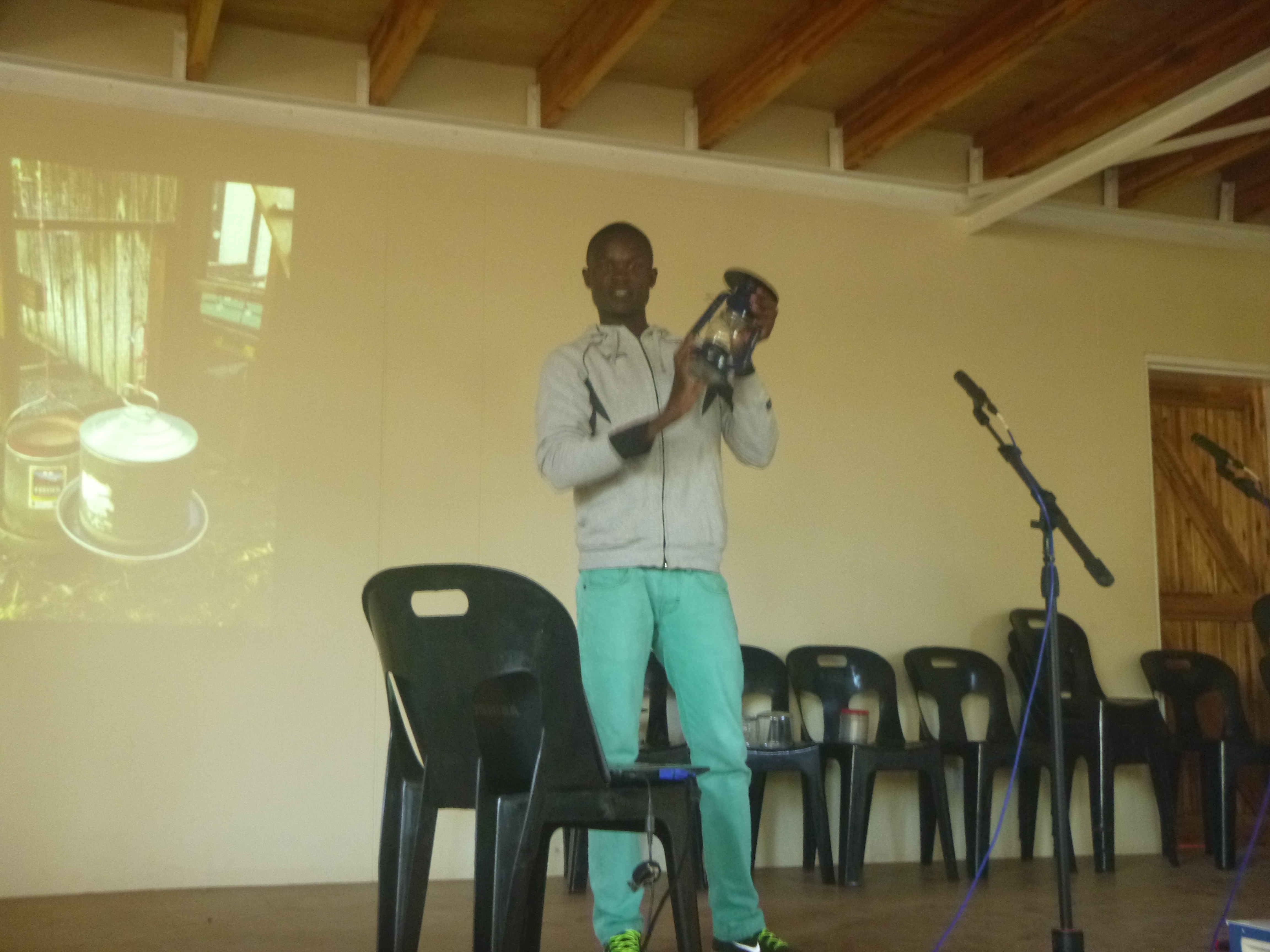
We were treated to two performances from the school’s student a cappella groups. The boys gave a spirited rendition of “The Lion Sleeps Tonight,” and the girls a beautiful song called “Malaika.” Then the director of the school called up two students to talk about projects the students had been working on. The first boy proudly presented cubes of tightly packed used water bottles that were lashed together with recycled plastic. He demonstrated using them as chairs, tables, foot rests, and when he lined them up, a bed. The next student showed off one of the solar lights he had made using old tin cans and plastic peanut butter jars. The beauty of this project is that the students made enough solar lamps so that every child who attends Jacaranda can take one home with them to study at night. (Considering it gets dark here around 5:30 p.m. and electricity is not always reliable or available, the solar lamps are a real game-changer for these students.)
The plastic bottle cube project. (I apologize for the poor picture quality!)One of the Jacaranda students, Charles, presenting a solar light.
After all the Jacaranda student presentations, the 9 of us went up on stage. Just introducing ourselves with what we studied and where we were from garnered applause. (We later found out from the school director that the students’ understanding of engineers was limited to people who work on cars, so it must have been really exciting for them to meet students studying biomedical, electrical and industrial engineering.) Christina took the lead and talked about the work we’d been doing with the phototherapy dosing meter, but ended her speech with a few words of personal advice for the girls in the crowd who are decidedly underrepresented in Malawian higher education. (Christina is one of 3 female electrical engineers in her class year at the Poly. There are no female mechanical engineers her year.)
Then we collectively gave overviews of the other devices we brought: the bCPAP and respiratory rate timer. When we finished, the school director opened the floor to questions, and dozens of students’ arms shot up. Because of the large age rage of the students, the questions varied quite a bit in complexity, (including, “Does the breath machine use electricity?” in reference to the bCPAP to, “Describe the calibration methods you used to increase the robustness of your phototherapy dosing meter,”) but all were equally brazen and hungry for understanding.
Francis closed out our presentation with some apt advice: “If you want to go fast,” he said, “go alone. But if you want to go far, go together.”
One of my favorite moments from the visit was an insightful parallel that Marie – the founder of Jacaranda – drew. She had just returned from a few week visit to Texas, and had witnessed the aftermath of all the recent flooding there. Certainly, Malawi experiences much more extensive and devastating flooding than Texas, but Marie noted that despite so many obvious differences between the two places, Texans and Malawians still experience some of the same problems, and in that way we are united. “In Texas, it flooded, homes were lost, people died. In Malawi, it flooded, homes were lost, people died,” she remarked, “We are the same.”She used this comparison to encourage and inspire her students that they could do anything they set their minds to.
The joy, hope and excitement at Jacaranda was contagious. At several points during the visit I found myself working very hard to hold back tears because of how inspiring it was. As we were leaving, we talked with the director to see if we could come back and chat some more with the students because we were all equally moved by the experience. Next Friday we’ll be going back to give a mini engineering design workshop for any student that wants to attend. (And after last week’s receptions, I get the feeling there will be quite a few very eager students in attendance.) I can’t wait to go back. In a way, it is unrelated to our internship in Malawi this summer, but at the same time, I think it couldn’t be more relevant. The spirit and mission of Jacaranda are beacons of hope, and I believe it is equipping its students to be the future leaders of a better and brighter Malawi.
My last post was pretty big picture- definitely information that I wanted to share, but nothing that inherently unique to my experience at St. Gabriel’s. Therefore, this post is going to be basically the polar opposite. This past week has been chock full of surprises- lots of interesting opportunities to learn and to serve. At the same time, Nkechi and I have agreed that it seems like we’re getting into a rhythm here. We’re on friendly terms with a fair number of the hospital staff, and for some strange reason, it seems like they like us! I think that it’s this familiarity that is opening doors for us- now that people see that we’re in it for the (relatively) long haul, our friendships are transforming into partnerships (and vice versa). The result has been our most exciting week yet!!! Here’s a brief peek at what it’s held so far:
Lunch with a nun (yeah, my Monday was cooler than yours)
On Monday morning, we were going about our business of preparing for the week when we came face to face with Sister Justina. St. Gabriel’s resident superhero, Sr. Justina has spent 50 years in Namitete, raising the hospital from the ground up and expanding support from her order in Luxemburg. At one point, she was placing IVs by candlelight in a 2-room clinic. You know, casual. We weren’t as much invited as instructed to come to lunch that afternoon. And it was great! No, not just because I got to have lunch with a nun. Sr. Justina truly is the authority on Namitete and the hospital, and we benefitted immensely from her experiences and her complete honesty. She told us point blank that one of our ideas wouldn’t work, which was refreshing and some valuable insight from a woman who has been there, done that.
Watching my first C-section (since my own)
Monday night, we spent some time on night duty with one of the clinical officers. Again, this was thoroughly unexpected- we were just starting to cook dinner when the phone rang, and we were asked if we wanted to watch a C-section. Eating took a backseat to opportunity, and we rushed over (one of the benefits of living 1 minute away from the hospital). I was surprised by how clean it was. Not the operating theater, since I was already aware of the measures taken to maintain the sterile field. Rather, I was surprised by how straightforward the procedure appeared. The incision was made smoothly, exposing the uterus fairly quickly. After a few minutes of maneuvering, it was just a matter of making a quick incision and then BAM! The baby’s head appeared. The whole process of removing the infant occurred so quickly and smoothly that I gasped audibly when the child appeared. The neonate was not breathing upon delivery, and as they were whisked to Labor Ward I was reminded of why so many of BTB’s technologies exist (and what our objectives are for the future). But the procedure itself was still unbelievable- I feel like the whole ‘miracle of life’ thing isn’t such a cheesy description of birth after all.
Hands-on teaching in Palliative Care (Morphine Tracker’s maiden voyage)
This week we had our first student! Collins is a member of St. Gabe’s palliative care team- although he (and everyone else we will be working with) has responsibilities throughout the hospital, he has been identified by Alex (the main Palliative Care nurse) as a potential ‘point person’ for the use of our software. We spent around an hour each day showing him the program and practicing. It’s been a really great way to identify potential roadblocks in future trainings or in the software itself. I also completely understand why Alex has recommended Collins for this job. He is a fast learner, devoted to the task, and has an unendingly positive attitude!
Family centered care unit on a clinic day- these are our patients for palliative and ART (HIV treatment)
Taking a hot shower (yes, this is important enough to be on the list)
It was my first hot shower in a month. Hair was washed. Deities were praised. All in all, a pretty big moment.
Seeing Malawi’s premier incinerator (AKA only incinerator)
I think that we must be sending off some sort of sonic signal telling people to befriend us, because one afternoon, a man we had never met knocked on our door. His name was Happy, he told us, and he runs the hospital’s incinerator. Would we like to come see where he worked some time?
When someone randomly shows up at your door and asks if you want to see an incinerator, there is only one thing to do: say heck yeah.
We learned from Happy that St. Gabriel’s has the only incinerator in Malawi. While I have been unable to verify this fact, apparently their system is so comparatively advanced that they burn trash for hospitals in Blantyre and the American Embassy in Lilongwe! This tidbit raised some important concerns about waste management in Malawi- apparently, most hospitals dig pits and simply dump their waste (including delicate/organic materials such as post-surgical materials, placentas, and amputated tissues). In contrast, St. Gabe’s system allows for the complete combustion of materials, and the smoke filtration ensures low toxicity for the surrounding area. Although it may not be as glamorous as other areas of the hospital, it was still a great opportunity to understand medicine as a process that starts before the patient enters the doors and ends with the disposal of byproducts of their visit. Waste disposal seems like such a low priority, but when you consider what would happen without it, the process seems anything but trivial.
Morning rounds in the male ward (venturing into uncharted territory)
Wednesday, we snagged Gift (one of the clinical officers) to show him some BTB technology. After we finished, we stuck around for our first real experience with Male Ward. Male Ward tends to be somewhat of a mixed bag, more so than paeds (mostly pneumonia and malaria) or female (pregnancy or abortion-related, mainly). We had chances to see typhoid, probable tuberculosis, HIV, stroke, pneumonia, heart failure, psychosomatic illness, and diabetes (both types). Working with Gift and Jason, a medical student from New Zealand, gave us tremendous insight into the marriage between patient history and physical examination. It was also interesting to see how they managed patients who were in male ward for the long haul. Especially alarming, it seemed that the diabetes patients were there for the longest periods of time (almost a month for one man!) Diabetes management (which I touched on in my last post) is a complicated problem in Malawi, and seeing such gifted clinicians struggling to stabilize patients’ glucose sparked a desire to learn more about the roles of technology and policy in addressing the problem.
An ‘American Feast’ (if we dare describe our cooking as such)
Tonight, we repaid a favor to our friend Bright, who is a clinical officer. Bright was kind enough to invite us into his home for nsima with beans, a delicious piece of Malawian culture. We decided to in turn invite him for an American feast at the Zitha House! After a lengthy debate about what constitutes American food, we decided to prepare green beans, mac n’ cheese, fried chicken, and vanilla pudding (the last of these at Bright’s request). They may not have tasted just like home, but we had a great time showing our friend how to cook American specialties, learning some more Chichewa, and swapping stories.
An obligatory pre-feast selfie during part 2 of our Malawian/American cultural exchange
This doesn’t even come close to being a comprehensive list of our week’s accomplishments! We’ve had some great experiences getting tech feedback from the hospital director, learning about device repair from the maintenance manager, playing with neighborhood kids, and preparing for our full-scale rollout of Morphine Tracker! And the best part is that our week isn’t even over. This weekend marks both the American and Malawian independence days, so I’m sure it will be one for the books. Keep on the lookout for more updates soon, but till then, tionanna!
Guidelines are a pretty big institution in the field of medicine. They help doctors identify a course of treatment or set the baseline for the standard of care for a certain condition. They are usually developed after much research and experimentation. They are widely respected in the medical community. The problem is that most of these guidelines just don’t work in low-resource health settings. In conversations with doctors and nurses at Queens, there have been quite a few instances that have illustrated how guidelines go awry on the ground.
APGAR Scores
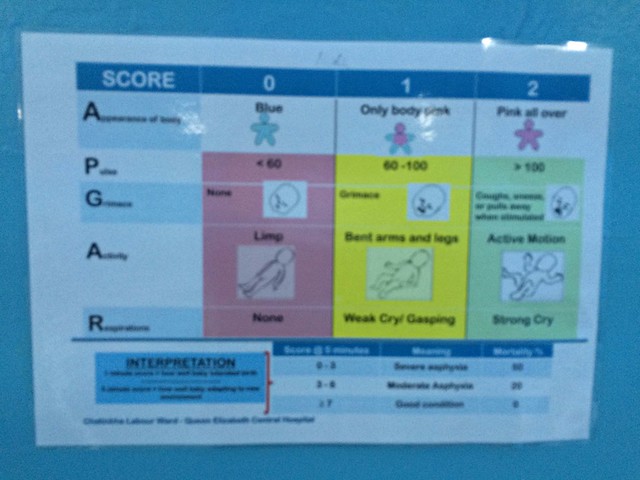
APGAR scores are used to rate the condition of a baby 1 and 5 minutes after delivery. APGAR is an acronym for Appearance, Pulse, Grimace, Activity, Respiration. In each of these categories, the baby can get a score of 0, 1, or 2 depending on how well they’re doing. Here’s a (somewhat blurry) picture of APGAR guidelines posted in the Maternity Ward.
APGAR scores can be useful in identifying the health status of the baby, but at QECH, given the high volume of babies with Respiratory Distress Syndrome (RDS) and Birth Asphyxia, APGAR scores are often irrelevant and aren’t recorded very consistently. Babies who are blue and barely breathing spur the midwives into action as they try to save the baby rather than record an APGAR score. This doesn’t mean that they’re flaunting protocol on purpose. Rather, it means that they are overstretched and usually don’t have the time to consider APGAR scores when there are multiple complicated deliveries happening at the same time.
Putting Patients on CPAP
Infants with RDS are generally supposed to be put on CPAP. However, a lot of hospitals with the Pumani bCPAP have subpar rates of infants with RDS who are actually put on CPAP. At the CPAP coordinator meeting, some of the coordinators mentioned that CPAP isn’t used in their hospital because nurses feel uncertain about the machine despite detailed guidelines from the CPAP Office about when and how to use the device.
More worrying, however, was one presentation from Kamuzu Central Hospital (KCH). The coordinator from KCH said that the Pumani CPAP was not used at all in the month of January because a few foreign doctors did not think the machine worked effectively (based on their expert opinion rather than evidence), and did not put their RDS patients on CPAP. Though these doctors were eventually convinced of the benefits of the Pumani, this situation highlights a serious problem. Both Alfred and Norman (our Ministry of Health partners) harped on the lack of national guidelines on the standard of care for certain conditions. They explained that each hospital largely sets its own guidelines. This makes it easier for visiting doctors to question the system and try to change practices that have been proven to be effective and useful on the ground.
NICE Guidelines for Inducing Labour
One of the most interesting and challenging dilemmas I have heard about during this internship concerns the practice of inducing labour in mothers. Last week, we got the chance to sit in on a Maternal and Child Mortality Morning Meeting–a special session where doctors from Paeds and Maternity came together to discuss best practices and areas of improvement. A big topic of conversation was the NICE Guidelines on labour induction, which outline the situations in which inducing labour is a good idea. These include a setting with adequate “safety and support procedures,” “facilities… for continuous electronic fetal heart rate and uterine contraction monitoring,” and “availability of pain relief options.”
The problem is that in the Delivery Suite, many of these conditions cannot be met. Yet there are mothers who are post-term or have complications and need to deliver their babies as soon as possible in order to protect the health of both the mother and the child. These aren’t isolated occasions either. Often, many mothers in the ward on a particular day have to be induced. However, given the limited equipment and staff, inducing all of these mothers at the same time can also be a disaster. It’s a fine balance. On the one hand, clinicians don’t want to induce labour unless they know they can give mothers an appropriate level of individualized care. On the other, not inducing these mothers could lead to more complications and bad outcomes for all parties involved. It’s a dilemma that makes the NICE Guidelines a nice guideline, but an unhelpful standard in a ward that has its hands tied by a lack of resources. Instead of looking at the guidelines, nurses and clinicians make their decisions on a case-by-case, day-by-day basis–a method that is occasionally successful and always stressful.
Yesterday, Karen and I travelled to Lilongwe (the capital) with the CPAP Office staff to attend the CPAP Coordinator Meeting. This meeting is an opportunity for the district coordinators for the CPAP project to come together and talk about the progress of CPAP implementation at their respective hospitals. Just before the morning tea break, Norman, our Ministry of Health point person and ARI Programme Coordinator, exclaimed, “Data is Power!” It’s from his bold statement that this post gets its title.
The CPAP Coordinator Meeting is all about data visualization. Every single coordinator is expected to present data about the use of CPAP and the rates of neonatal survival in their districts. It is meetings like this that help make the Rice CPAP project a beneficial effort. Economist William Easterly writes in his book The White Man’s Burden that most aid efforts lack a system of adequate feedback and evaluation, which leads to a disconnect between donors, implementers, and end-users. The CPAP Coordinator Meeting addresses exactly this issue by fostering communication between CPAP project staff and the people who are implementing the project at the district levels. The presentations are impressive–coordinators aren’t afraid to admit that there are weak spots in their implementation efforts and they are happy to put forward solutions and ideas to help their colleagues.
Discussion at the Coordinator Meeting featuring a Portrait of Prof. Arthur Peter Mutharika
Despite the merits of this conference of coordinators, what is equally evident in the meeting is how hard it is to collect, record, and archive data in an accessible way. Numerous presenters talked about how entire months of data on neonatal mortality rates were unavailable to them because of missing logbooks, locked storerooms, insufficient monitoring forms, or incorrect data entry. It makes evaluation extremely hard, especially since the CPAP project is now operating in almost every Malawian district. Each district and each hospital is independently in charge of recording data, which makes it easier for human error and logistical malfunctions to corrupt data collection. Norman’s exclamation this morning was in response to the fact that hospital after hospital came up to present only to show missing data or poorly collected metrics. His frustration is definitely warranted. ‘
The final piece of the breakdown in data collection is the lack of reliable communication technology. In several districts, supplies and data collection materials were in short supply mostly because district coordinators failed to contact the CPAP Office in Blantyre in order to inform them of the situation. In other instances, broken CPAPs were left unfixed for months because of miscommunications. There are shaky channels of communication between district hospitals, PAM, and the CPAP team, which adds another barrier to effective data management.
The CPAP project is extremely good at training, motivating, and following up with district-level data collectors. However, there are inherent obstacles int he Malawian healthcare system that hinder evaluation efforts. Once again, this is an opportunity for an EMR system to be effective. It would prevent data loss and could aid in communication, making research on healthcare interventions far more feasible. If data is power, then EMR systems are keys to the kingdom, since they will open up a whole new realm of easy data collection and management.
We are nearing the halfway point of our internship, and have transitioned from the first round of projects onto the next. Here is a brief update on some of our main focuses this summer:
Phototherapy dosing meter. I’ve written about this technology extensively already on this blog, and am happy to share that it is now completed. The device was tested using the standard of care in the States. The preliminary testing showed a 3.7% error for our device, but the new technology costs almost $2000 less than the standard. We’ve also completed extensive documentation on the new technology, to facilitate further testing and development. We will be taking the completed device to PAM and QECH soon, to get final feedback from professional engineers and nurses on the prototype.
Suction pump attachment piece. This is the second design project we are pursuing as a team, and are currently between the brainstorming/planning phase and the prototyping phase. The idea for the project came from PAM (who fixes the broken devices from the hospital), and we look forward to involving them throughout the design process. The impetus for the creation of this new technology was the common malfunction of suction pump machines, in which the collection bottles overflow, backup into the machines, and cause permanent damage. Our device will ring an alarm when the collection bottles are ¾ full, and automatically shut the machine off when it reaches capacity. This prevents backflow into the machine, which is a cause for many dozens of suction pumps to be sent to PAM. We plan to have this prototype finished and tested within the next few weeks.
Rice and Polytechnic website. Inspired by the relationship that developed between us interns, we decided to build a website to facilitate further interaction between Rice students and Poly students (that won’t require a 35 hour travel day). The website we are building allows for students from either university to give feedback on current design projects being worked on. Additionally, general questions that may have answers sourced from the alternate country can be posted to this website. Hopefully, both student understanding and technology design will benefit from this interaction.
Orientation week. We’ve created a time table for the orientation week we are helping to plan, which will take place the first week of August for first year Poly biomedical engineering students. So far, the week is shaping up to be really fun. Currently, we are working on nailing down speakers for a few lectures, as well as creating our own content for some lectures the interns will put on. After that, we will focus on creating a week-long design project to introduce students to biomedical engineering. Planning for the orientation week will be ongoing throughout the rest of our internship.
There are a few other projects in the works—including preparation for a faculty design workshop in late July, and creating the engineering-focused activities for students at Jacaranda—which we look forward to focusing on in the coming weeks!
Voting/discussing what projects we will pursue for the remainder of our internshipBeginning stages of suction pump attachment circuitOld bottles from broken suction pump machines in PAMTesting equipment for the phototherapy dosing meter
Through the past four weeks, working nine hours a day and five days a week together, we seven Poly interns have gotten really close. In addition to the many practical benefits that this relationship has provided, it has also been the cause of a lot of laughs through discovering various cultural differences. Here are a few of the topics that we’ve found particularly entertaining:
Dancing. The Malawian interns never get tired of making fun of our (as they claim) poor dancing abilities. In our defense, dancing seems to be a far more integral part of Malawian culture than it is American culture; in public spaces, it’s rare to not hear music playing and see someone dancing a bit (Tanya wrote a good blog recently about the songs of Blantyre, if you’re interested). At first I thought the interns were just giving us a hard time about our dancing skills, but their sentiment was recently reflected by an unbiased third party. We attended a wedding this past weekend—the nephew of a professor at the Poly was getting married, and the prof kindly invited us—which was a ton of fun. There were a few hundred attendees, all of whom sat in chairs facing the stage where the bride and groom sat. For about 2.5 hours, a tradition that we have dubbed “money dancing” ensued: various groups are called out (ex: family of the groom, friends of the bride, those from the groom’s village) to rise from their chairs and move forwards to dance around the bride and groom, while tossing small bills towards the couple. Generally, the groups were each a few dozen strong, and filled with the impressive Malawian dancers. Unfortunately, Tanya, Catherine, Emily, and I were the only four Americans in attendance. So, when the MC called out for all Americans to rise and dance about the bride and groom, the four of us alone had to put forth our best efforts and embrace the money dance tradition. I thought we were doing pretty well, until we were asked (with 100% sincerity and kindness), “Are you tired? Is that why you’re not dancing well? Do you need to sit back down?” It was then we realized the interns hadn’t just been giving us a hard time—Americans have a thing or two to learn from the Malawians about dance.
Santa Claus. Prompted by some questions about American Christmas traditions that Francis had asked, I found myself attempting to explain the common story of Santa Claus. It was very difficult to find words to explain the reason for a collective, nation-wide lie that is annually passed down from parent to child. Making this even more difficult was the fact that this lie revolves around an unknown old man sneaking into homes at night through the chimney. However Christmas wasn’t voted “the weirdest” of all American holidays—that title was reserved for Halloween.
Food. New foods—both from Malawi and from America—are always exciting to try. For the American interns, we’ve grown addicted to mendazi, which are delicious, fried, dough balls. For the Malawians, a favorite has been banana bread, which Emily, Catherine, and I cooked a few weeks ago. It was very well received—though was renamed “banana cake” by them—but unfortunately has also inspired a never ending craving for the treat. Whenever we are trying to convince the interns to do a favor for us, their answer is now perpetually the same: “You know the terms.” The terms are always banana cake.
American TV. The Malawian interns often reference various American TV shows and ask, “is it really like that?” One show that provided some significant cause for distress was the Bachelorette.
Of course, the similarities and differences in our backgrounds—as well as what we are learning from one another—run deeper and are more significant than what I’ve listed above. But these are a few of the little things that make us laugh, allowing us to grow closer and learn more than we would be able to otherwise.
Our mendazi supplier; the dough balls are visible in the front right bucket with a green lidChristina using the bCPAP doll to show us how to carry a baby Malawian styleLaughter ensuing as Catherine showed Francis up at an arm wrestling matchCharles sharing some Malawian dance music with EmilyA shot from the wedding; the group you see at the front is currently doing the money dance as those sitting down look on