A few common refrains in the world of development-focused, service-minded people include “making a mark” and “creating change in the community” and “impacting individuals”. These alliterative idioms may sound attractive, but they encompass a dangerous mindset. Beginning a two month internship with the goal of changing things would have prevented me from being able to learn from, adapt to, and understand the cultural, social, economic, and health contexts that I was about to be immersed in. Reflecting back on this experience, though, I have to admit that marks have been made, so this post is a catalog of the scars, bumps, bruises, and more that I’ll leave Malawi with.
Stubbed toes and hole-ridden shoes
I am by no means the most graceful person, as any of the other interns can attest. The uneven ground around Blantyre often had me tripping around the city as I took in the sights. I had less of an excuse for my clumsiness at Queens. My interest in peering into wards and out through windows often led me into walls and doors, causing me to stub several toes in the process. There were too many colors, smells, sounds, and sights for me to watch where I was going (or at least that’s what I say to save face). By the end of the internship, I was much better at walking the familiar routes in the hospital. I’m going to miss the long walk between the CPAP Office and Chatinkha Nursery, which we sometimes took several times a day. It was probably this trek more than anything that created and widened the ever-growing hole in my shoes.
Papercuts from folder-making
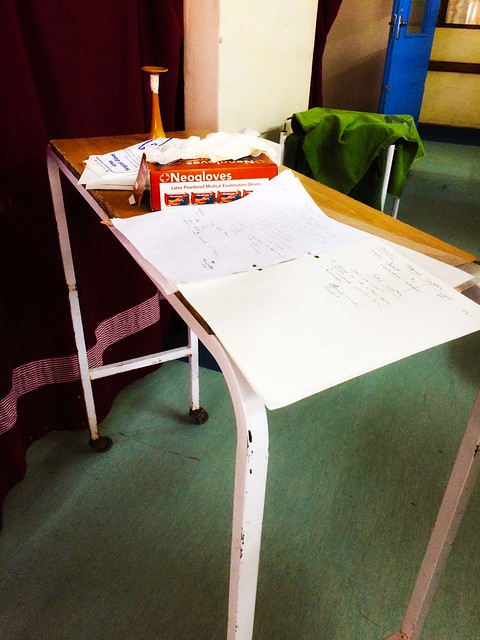
Making folders for the maternity ward was one of the smallest but most rewarding things we did. We noticed early on that the ward needed chart holders, which led to several hours of hand-lamination that left me with some pretty painful papercuts. The best part was being able to follow up on how the chart holders were doing. The nurses and doctors in the ward often recognized us as the “yellow-folder girls” and always welcomed us back with huge smiles and excited chatter about how they were using the chart holders. It was great to see the effect such a small project had on the ward. Don’t get me wrong. We didn’t change lives or make an impact in the traditional sense, but we did make the jobs of clinicians in the ward just a little bit easier. Earning their smiles, interest, and excitement was a great reward.
A semi-permanent dust tan
My personal project during this internship was to learn more about the supply chain of medical devices as it related to the Ministry of Health, Physical Assets Management, the Department of Procurement, and QECH. The best part of the project was being able to talk to a wide variety of people for my research. From contacts in the MoH in Lilongwe to officials at QECH, I talked to a diverse range of people who were extremely welcoming and willing to answer my litany of questions with the utmost honesty. Last Friday, I got to run around Blantyre between QECH, the College of Medicine, PAM, and copyshops as I asked some of my final questions. It left me exhausted, excited, and covered in a fine layer of dust from traipsing across the city.
Scars from playing soccer at Lake Malawi
Visiting Lake Malawi was probably the pinnacle of our cultural immersion in Malawi. We travelled up with the Malawian interns and did everything typically Malawian: eating Kampango (or butterfish), learning to play Bawo (our new favorite game), speaking Chichewa with the villagers. On the rocky shores of the lake, there were roving bands of children (and I do literally mean bands), who played us ridiculous and infectious versions of “Who Let the Dogs Out” and other classics. At one point, we invited the children to an impromptu soccer game (barefoot, of course) which left me with scars all along my feet.
In the end, Malawi probably made more marks on me than vice versa. I’ve learned and experienced more in these two months than I could have ever hoped. I come away with more knowledge about Malawi, a renewed respect for the healthcare professionals who work tirelessly in low-resource settings, and an appreciation for the complexities and challenges of the healthcare system itself. Nearly every intern blog from previous years has ended with a “Tionana” (“see you later” in Chichewa), and I definitely understand that sentiment. I don’t want this internship to be a one-off experience. I want to come back to Malawi, to low-resource health settings, to other countries so I can learn more and do more. I’m not out to make my mark on the world, but rather I want to be marked by my travels, experiences, and knowledge so I can be an advocate for and an agent of sustainable change.