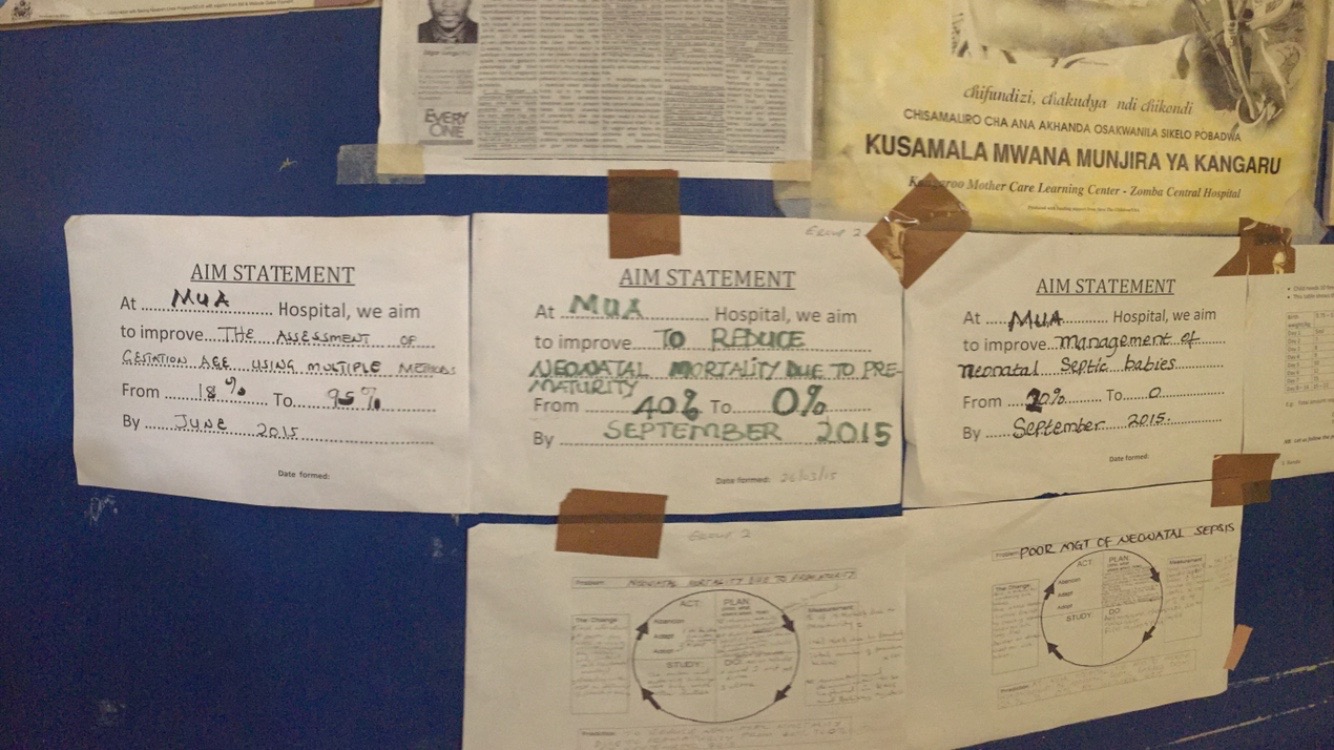
One of my individual projects is a qualitative analysis of the CPAP mentorship program at district hospitals. Basically, very well-trained CPAP nurses from Queen’s go to struggling district hospitals to mentor nurses and staff on CPAP. From this visit, the mentor’s write a report on each mentee’s performance and improvement, as well as a general report about the neonatal ward in the hospital. So what I do is, go through all these reports and code various trends that I find pervasive across the hospitals to help to give more information on the condition of the nurseries, adherence to CPAP procedures, and if the mentorship program is effective, which informs the CPAP team about how to improve the mentorship program. I draw information from these reports, as well as personal interviews with the mentors here at Queen’s.
Okay, all the technical stuff is out of the way.
Let’s talk about how all this data collection and analyzing gave me goosebumps. Surprising, no?
Yesterday, I interviewed a veteran CPAP nurse from Queen’s named Chrissie. I told her about my project, and we worked out that 2pm is the best time to conduct the interview. Being in Malawi, things often seem to run on their own clock, so I knew 2pm could mean anywhere between 2pm to… well, anytime this week. Chrissie comes into the office at 1:50pm with a stack of reports from all her mentorships compiled and ready to go. One can say I was caught a little off-guard. So, I ask my questions, she gives me thoughtful, insightful answers. I can tell when she talks about her work that she is completely committed and believes in what she is doing. I see this commonly among nurses here, but still every time I come across it, I’m inspired by their dedication. As the interview was coming to a close, we were getting up and putting our things together to go our separate ways. I asked her what she had going on the rest of the day, and she told me she was on her way to teach a CPAP refresher for the nurses in the pediatric nursery and she was so excited. I asked her, “You really love CPAP, don’t you?” to which she responded with, “CPAP is why I do what I do.” From there she told me all about what CPAP means to her and this hospital.
Chrissie told me that she goes into work each day and mothers waiting in the hallways recognize her as the CPAP nurse. “Mothers come up to me and say [cradling her arms as if she was holding a baby] ‘Do you remember me? You are the nurse that saved my son’s life.’ ‘You’re that CPAP nurse! Look at my girl, she’s healthy and alive! Thank you, sister!'”
Then she told me about a time that MBC, the major news broadcasting company in Malawi, was interviewing patients at Queen’s. One of the interviews was with a mother that had recently given birth to a preterm baby that had to be put on CPAP. “In the news cast, this lady said, ‘My son is alive and breathing because of the endless care of the amazing nurse, Chrissie Mbendera.’ My name! On the news!”
After I was fully in awe of everything about Chrissie, she told me a story about when she was shopping for potatoes at the market. She told me that it was some random weekend, and she was buying potatoes from a vendor at the market. “I told the woman, ‘I would like one bunch of those over there.’ Then, I felt a person come up behind me and put my hand on my shoulder. This person said, ‘No, she wants two bunches and I am buying them for her. This woman saved my baby boy’s life.'”
Was I wrong about the goosebumps?

The new Chatinkha nursery in QECH.
http://www.rice360.rice.edu/#!day-one-project/udbk5