Welcome back to my blog! It’s been a very eventful weeks in which I visited two hospitals, traveled to Lilongwe and back for a pitch competition (and got a broken tire on the journey), and hiked a small mountain (or rather, a plateau) on our weekend adventure (while unknowingly having a fever). In an effort to keep my experiences on this blog in real time, this will be a three part blog (four if counting the customary fun photos section) featuring the highlights of what I’ve learned over the last two weeks.

Part 1: A Small Glimpse at What it Means to be a Doctor
Kyla, Liseth, and I have had the opportunity to attend to the daily handover meetings of the pediatric department at QECH, in which the doctors on call for the night shift inform the other doctors on new admissions and deaths that occurred in the various wards during the night. The first meeting I attended occurred on a Friday, on which the mortality report for the week is presented. Each case was displayed as a row on the spreadsheet with a patient number, a date of admission, a summary of symptoms, and laboratory test results. Initially, this information seemed so abstract—just tiny black text on a white screen in a dimly lit room. Then, it hit me.
Our path to and from the CPAP office passes a busy intersection that contains, among other things, the path between the pediatric wards and the morgue. The week prior, we saw a stretcher with white sheets covering the faint outline of a small body being wheeled along this path followed by a line of bereaving family members. In that moment, I realized that that small body could have very easily been any of the data points displayed on the projector, and it deeply perturbed me that patient—that child—could be simply turned into a collection of clinical criteria. The doctors’ discussion of these cases augmented this effect, picking apart the symptoms they witnessed and treatment details.
At one point, there was some confusion over which case was being discussed due to the symptoms being fairly common. Then, one doctor exclaimed, “I know who you’re talking about,” another doctor echoed, “the one with…,” several others nodded in confirmation, as if there was something more memorable than symptoms about this patient that was etched into their minds. Then, I understood: Being doctors, they had to simultaneously recognize the humanity of each of their patients in and think of them as cases whose symptoms had to be solved and, in the worst case scenarios, whose deaths had to be learned from to prevent similar ones in the future. Sometimes, it seemed, these two aspects were in direct conflict with each other, and like the doctors in that room, in my future, I will have to handle the precarious yet crucial balance between them.
Part 2: More Thoughts on Implementation
One of the things my team in the GLHT 360 course initially struggled with when designing the Ballard Score training model during the semester was envisioning a role for it. During our research process, we repeatedly learned that the Ballard Score was seldom, in practice, used to determine gestational age, and we struggled to see how a training model could change these established norms. The missing piece of this puzzle that we weren’t thinking about was implementation: obviously a training model by itself couldn’t compel healthcare providers to use the Ballard Score, but with proper implementation, it could be a key part of the process to encourage increased use.

The visit to QECH two weeks ago (along with the visits to Zomba Central Hospital and Mulanje District Hospital the first week) truly allowed me to envision how, at least hypothetically, implementation of the training model could work. At QECH, we met with student nurses in their final year of nursing school, and they, along with Prince (a nurse in the NICU who works with Rice 360), explained how training for the Ballard Score currently works. In short, during their unit on prematurity, for a few hours on one day, they are given a presentation on the Ballard Score, and, at best, the instructor demonstrates the neuromuscular signs on a normal baby doll at front of the room. However, there are other procedures that they practice on baby models during skills labs in nursing school, and I think it would be possible to incorporate the Ballard Score into a skills lab if an adequate training model were developed.

In addition, for nurses who have already graduated, this training model could be incorporated into periodic training workshops on the Ballard Score. From some of the checklists I read in the CPAP office filled in by national supervisors, I learned that trainings on other topics such as CPAP, COIN, and Helping Babies Breathe are currently held in hospitals throughout Malawi. Multiple nurses at all three hospitals also told us that they recognized the importance of the Ballard Score and, at least hypothetically, would attend Ballard Score trainings to be able to do the procedure more efficiently and use it more often. (This is in addition to the amazing app the team at the Poly is developing to make it easier to record ratings for the Ballard Score and thus reduce the time needed to perform it).
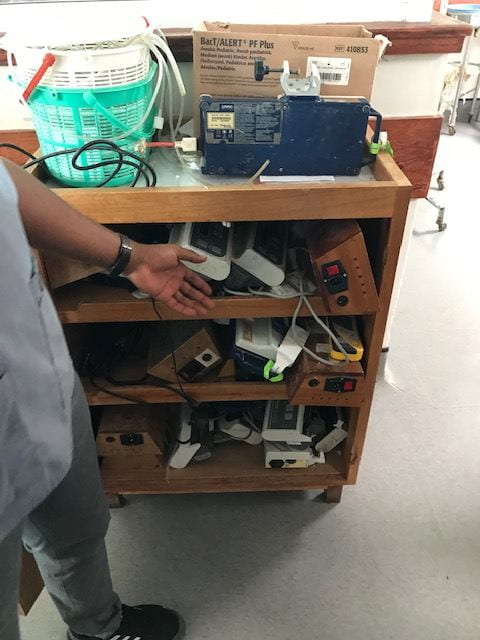
However, I fully recognize how far away this hypothetical implementation of the training model would be even in the best case scenario (though the Poly team is making amazing progress- they are determined to prototype five neuromuscular signs this summer and have started at least two already!). I was made even more aware of this during the QECH visit. Prince showed us a broken syringe pump in the shelf of old devices in the NICU and explained to us how important syringe pumps were in delivering fluid medications and how the fact it only worked with one size of syringe was troublesome. The fact that even Prince, who works for Rice 360, did not know about the syringe pump being developed by Rice 360 addressing these exact issues, even though it has already been in the prototyping process for a few years (I think?) emphasized just how long the process from needs finding to prototyping to clinical trials to manufacturing and implementation was. This made me appreciate the fact that the patients and maybe even the nurses and doctors that we meet on hospital visits aren’t going to be the ones who benefit from the technologies we develop based on their feedback; technology development and research in general doesn’t really solve the problems of today but those of tomorrow.
Part 3: An Overarching Theme in Needs Finding

Our visits to the nursery ward a QECH and to the Physical Assets Management (PAM) department at Kamuzu Central Hospital in Lilongwewere amazing opportunities for needs finding. Hearing two contrasting perspectives—the nurses that serve as the users of the devices and the biomedical engineers that are responsible for maintain them—successively was both intriguing and informative. There were definitely some differences in their views of the challenges that they face with medical equipment (viewing pre-set settings of suction machines as a benefit vs an obstacle, seeing the failure with temperature as user error vs a flaw in device design). Nevertheless, a lot of overarching themes emerged.
The theme that stood out most to me, that I had somewhat picked up on at Mulanje DHO and Zomba Central Hospital, was the constant scarcity of consumables. By consumables, I really do mean all types of consumables: plastic tubing of all kinds, stationary (both normal printer paper and special types of paper), test strips, etc. You name it, if it is meant to be used only once, there is definitely an issue of lack of availability with it. The consequences of this became apparent:
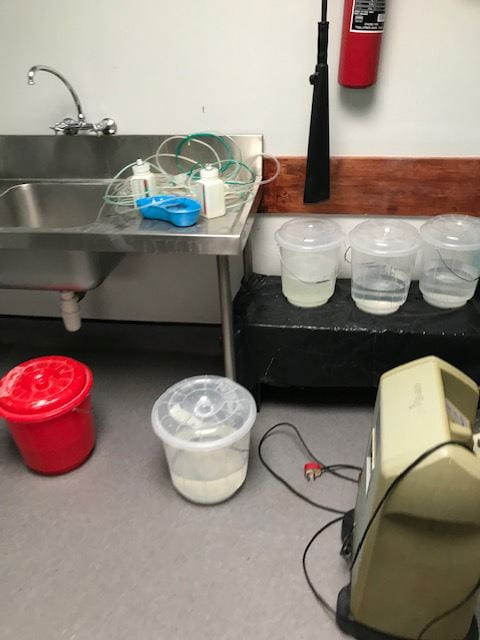
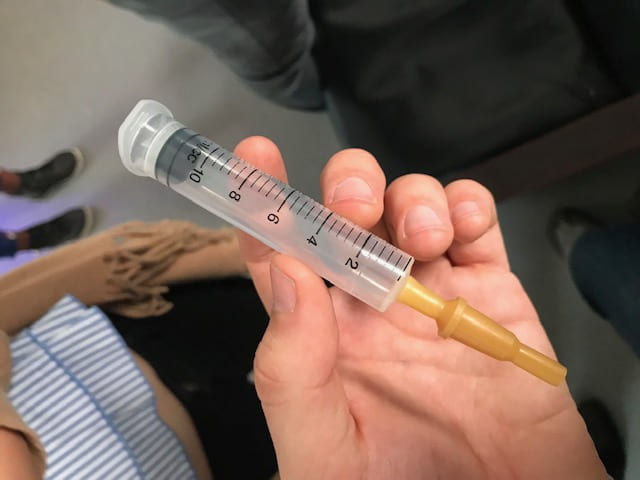
To make up for the lack on consumables, many disposable devices are re-used after sterilization with chlorine. While this is a clever and necessary work-around in these lower resource hospitals, it does not come without unintended effects (in addition to the clear possibility of insufficient disinfection). For instance, after sterilization, plastic suction tubes change texture and are more likely to cause trauma when inserted in an infant’s trachea, and the labeling on syringes used in feeding sets fade and then disappear, leading to less accurate measurements. When certain types of disposables aren’t available at all, sometimes other similar disposables are used in their place (suction tubes in place of oxygen tubes, components of IV sets for feeding sets). However, some consumables can’t be re-used or replaced—such as glucose test strips and hemoglobin test strips, and when these aren’t available, the critical functions they provide simply aren’t fulfilled.
While the scarcity of consumables may be, in large part, a distribution problem, I think there could be engineering design-based solutions to help address the issue—namely, creating versions of products that are meant to be reused. While, at least in my experience, the motivation behind designing reusable products is to reduce overall cost, it also ameliorates the difficulty of needing to continuously re-stock supplies. Looking beyond this, as suggested by Dr. Bond—the GLHT 360 professor that reviews all of our project ideas, designing better systems of sterilization that ensure more thorough disinfection or are less harmful to the material could fulfill part of this need, allowing some existing “disposable” devices to be become truly reusable and thus more compatible with the setting.
Overall, the last two weeks have allowed me to glimpse into the future—my personal future as a doctor, the future of the Ballard Score model, and potential for developing future technologies—with both hope and excitement but also an heightened awareness of the challenges that lie ahead.
Part 4: Fun Photos from This Week’s Adventures





-Sally