The past week has been a great one. Over the weekend Catherine, Emily, Sarah and I went out for chitenje (wrap) shopping. We went to different shops. I liked the tour so much because they were overwhelmed by the chitenje varieties that we found. This weekend we are going to a tailor so that he can make skirts, jackets, dresses and trousers for them. After the chitenje shopping we went to the wood market. They bought different items in the market and they told me that they will give them to their friends and families as gifts.
We also went to Jacaranda School for Orphans. It is 30 minutes away from the Polytechnic. We went there so that we can motivate the secondary school students. I took the lead in the motivation talk. I felt so proud of myself because I was able to encourage my Malawian ladies that they can make it to the university and contribute to the development of our country. As you know the literacy rate for ladies in Malawi is low, and it is my desire that the few students that I have motivated should become responsible citizens of Malawi. I had a little chat with the girls after the gathering and I inspired them through my life story. I told them that they should work hard at school and make good friends. They asked me a lot of questions about university life and how I made it. I told them different courses that they can pursue when they pass their secondary school certificate examinations. I really look forward to seeing Malawian girls succeed in their education so that they do not have to rely on someone for their sustainability
Me( in Orange Jacket) and the girls sharing advices
Phunziro means learning in Chichewa. Which is exactly what my first couple weeks here have been like. Learning about new people, a new country, a new culture, and new technologies.
As stated in my previous blog, the other weekend, we went to Lilongwe to get new internet! And then on Wednesday, the day before our big presentation at the morning meeting, I dropped my laptop! Luckily, the hospital staff was kind and allowed a technician to fix it, but it’s still in Lilongwe right now. Thanks to Renata for letting me borrow hers.
A major theme of this trip has been me being shocked at both how many resources are present and how few resources are present. While our internet has been pretty fast and allows for Skype calls, back home in my small town, my family has been without WIFI for the past week. The hospital has an amazing ART software and program, but the X-RAY machine has been gone. Perhaps the most shocking was the diversity of the Namitete market compared to the Chipiku store in Lilongwe. I saw Tabasco sauce there from back home in Louisiana! There was also Cajun chicken pasta and Louisiana Fried Chicken in the restaurant we went to. We live in a global world, friends.
People have been asking me so much what I have been doing. Currently our average day goes something like this
7:00 AM- Wake up; eat breakfast
7:30 AM- Go to the morning meeting. The nurses from the night shift give a summary of the patients who have been admitted, died, and of the special cases. After this presentations are given by the staff on a relevant morning topic. This is we did our presentation on our technologies to the clinicians.
8:00 AM- 12:00 AM- Shadowing clinicians, watching surgeries, meeting with contacts, but mostly working on Morphine Tracker Improvements
12:00PM-2:00PM- Malawian lunch time is a little bit longer. You have to have time to go home and cook nsima. Renata and I try to eat nsima at least once a week, if not more. It actually taste exactly like Nigerian fufu, and you eat it the same way, with your hands!
2:00PM-5:00PM- More meetings, and working on Morphine Tracker.
5:00PM-10:00PM- Shower, cook dinner, eat dinner, play some pool, work on med school apps , watch some t.v. or read a book
All seven of us interns in Blantyre had the good fortune of visiting Jacaranda this past Thursday. Jacaranda is a primary and secondary school, attended by around 400 students; their school is doing incredible things, and I encourage you to read more on their website (linked below). Here are a few of the roles we took on during our trip to Jacaranda.
Visitors. When we first arrived on the grounds, we were treated to a tour of the campus by two sweet, young teenagers. Everywhere we went, we were welcomed with wide smiles and a synchronized greeting call (a tradition at the school); we even enjoyed a short concert by the two acapella groups on campus.
ClassroomsOur two tour guides standing in the computer lab, in front of the libraryStudent-kept gardensExtremely talented female acapella group
Audience members. We first watched a presentation by some Jacaranda students on what engineering projects they had been working on. One team of students had taken used water bottles and reconstructed them into sturdy and versatile furniture pieces; some of the water bottle furniture had even been decorated at the school in the arts program. Another project was the creation of solar powered lanterns. They were very cheap devices, fashioned from clear food containers, a few solar panels, and various reflective materials. What had initially begun as a small project with only a few prototypes expanded, so that every student at the school had created their own lamp to use to walk home, study, and read at night. These simple technologies made a huge difference for the children, and we were all impressed by them; the students were rightly very proud of their lanterns.
Showing off his water bottle furniture
Presenters. For our presentation, we talked to the primary and secondary school students about what tertiary school is like, what engineering is, what technologies we were working on, and how the devices help those in the hospital. I have to take a moment to brag on Christina and Francis, two of the Poly interns from Malawi, who had inspiring and beautiful advice for the students during our presentation. Christina connected with the students—especially the young girls in the audience—so genuinely, encouraging them to keep up with their studies and stay focused on what is important while being aware of what is not. The rate of girls who pursue higher education isn’t high in Malawi, and the number who pursue science and engineering is even fewer; it was nice to have so many female engineering interns up on stage for the presentation, and to see Christina become a role model for many of the students in the audience. Francis began his speech by reminding everyone that, “everything in science started out as something small.” He spoke to the importance of pursuing ideas that have the potential to improve problems, even if the ideas seem impossible. His advice to continue creating, despite limited resources and the nagging feeling that your efforts will not result in huge change, I think hit home with a lot of people in the auditorium.
Audience; both primary and secondary school students attended
Before we left for the day, we hung around to talk to some of the students. One boy in particular came up to me to ask for some electrical engineering advice. Despite having no electrical training, he had deconstructed some of the extra lanterns and mounted the solar cells on top of his roof. From there, he wired the panels through the ceiling and along the walls of his room, powering light bulbs and brightening his nights; his natural ability to innovate and understand technology was impressive. Many of the students had question after question about how the medical devices we brought with us worked, and what materials were required to construct them. A large number of girls conglomerated, asking about what us female interns did in tertiary school. When they heard Karen was pre-med, they were very excited—they too want to be doctors. So many of the students were curious about the prospect of engineering, and wanted ideas for projects to pursue. The interns all decided to come back to Jacaranda on Friday afternoons for the remainder of our time here, to hold engineering workshops and information sessions. I’m excited to go back—the students were so kind, curious, and eager. Hopefully this will be an experience that starts small, but as Francis indicated, grows into something much more important.
Christina surrounded by a cohort of eager young girlsCharles giving advice to secondary students
I’ve felt like I had a logical understanding of morphine use in Malawi for some time now. I’ve spent the better part of four weeks working in palliative care at St. Gabe’s, so I have the logistics down pat. The need for a software to track morphine use appeared pretty clear after reading last year’s intern blogs almost religiously. I’ve even watched patients get started down the path of palliative care while shadowing. As far as I was concerned, the need for morphine tracking software could be explained in about three sentences:
Problems like chronic heart failure, cancer, stroke, and advanced AIDS can’t really be treated in Malawi. As a result, patients who have these chronic conditions often enter hospice for pain management (1), (2). Morphine, the strongest pain management tool in the palliative care arsenal, is strictly regulated and hard to procure (3), so keeping accurate records is important to ensuring that patients receive their medication without interruption.
Simple as that. To quote my man David Bowie, “Wham, bam, thank you, ma’am”.
Until today.
We accompanied Alex, the palliative care nurse, on home based care visits today. When we came to the first patient, I had to stoop to enter the low doorway of the brick hut. Inside, the rooms were mostly bare. The focal point immediately became the low mat, the pile of blankets tucked in the corner. Everything was still, quiet except for the guardian’s murmured greetings. Once the community health volunteers had settled in, I could hear low moans coming from the pile of cloths. The guardian, a stoic woman of late middle age, gingerly sat on the corner of the mat and began to answer our questions.
The patient, age 42, was suffering from HIV and late-stage anal cancer, the latter of which had manifested as large pus-filled lesions. As the volunteers closed around the bed, I realized that my initial assumptions that the bed was just covered with rags were understandable. She couldn’t have weighed more than 70 lbs. Dull skin was pulled taut, enough that every bone in the woman’s body appeared visible. Each joint seemed ready to snap as she was positioned for examination. Every movement was accompanied by low, antagonizing groans. Even the act of being repositioned into a seated posture caused her to nearly pass out from the pain.
I have never in my life seen anyone look that frail, that utterly breakable.
It was decided that the woman’s morphine dose should be doubled. The guardian’s mental wellbeing was assessed, and then the visit concluded with a word of prayer with the patient.
After visiting this patient, I understand the emotional and spiritual implications of morphine treatment. Tracking morphine stocks isn’t just the difference between having a medication and going without. Because although I can dream that this woman’s quality of life will improve with an increased morphine dose, I cannot even begin to imagine what she would be reduced to without any morphine at all.
Palliative care will never be sexy. It doesn’t present the adventure of surgery or the warm fuzziness of paeds. But for the patient I saw today, morphine is a concrete realization of comfort and peace in her final days.
**Side note: I had no intention of writing this blog post. I actually had another one written and cued up and everything. But after today, this is what came out, so this is what you get. I hope it means something.
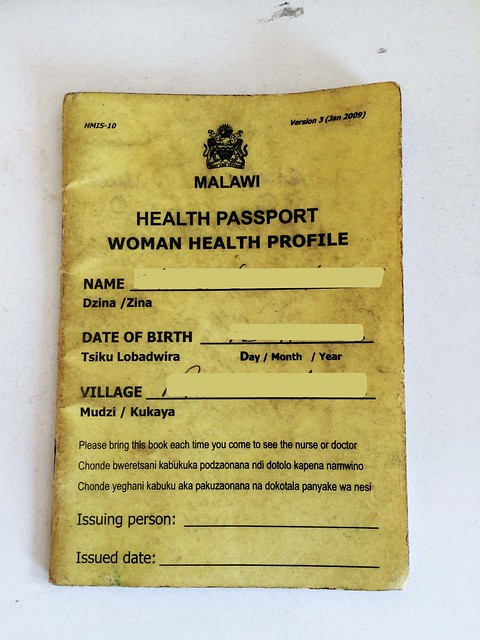
It’s not uncommon to run into foreign doctors in every ward at Queens. Since it is a teaching hospital associated with the College of Medicine there are numerous foreign doctors, visiting professors, and researchers roaming the halls. It’s great to have so many varied, international perspectives, but it also makes doctor-patient communication very hard. A lot of the patients at QECH know little to no English, and doctors’ inquiries into their complex medical histories are usually met with blank stares or detailed explanations in rapid Chichewa. So when their limited grasp of the local language fails them, the doctors flip through the patient charts and find the small, meticulously-kept, well-worn yellow booklets that act as windows into the lives and medical issues of each patient. These Health Passports are a health management information system that chronicles the check-ups, hospital visits, laboratory test results, and health conditions of each Malawian.
Health Passport from the Ministry of Health
Record of medical visit and the doctor’s notes
Given free to newborns or purchased for 200 kwacha (about $0.50) by everyone else, the passports are a great way to manage patient care collaboratively across institutions in the Malawian healthcare system. Since there are no standardized electronic systems that would allow hospitals to share electronic medical records (EMRs) with each other, the patient acts as the messenger, in charge of caring for and presenting the Health Passports at each medical visit.
It’s not always a perfect system. Often health centers forget to conduct routine tests or record the results of those tests in the health passports, which means doctors have to diagnose and treat patients using incomplete information. Yet, even with some holes in information, the health passports are invaluable in bridging language barriers and in providing a comprehensive report of patient history.
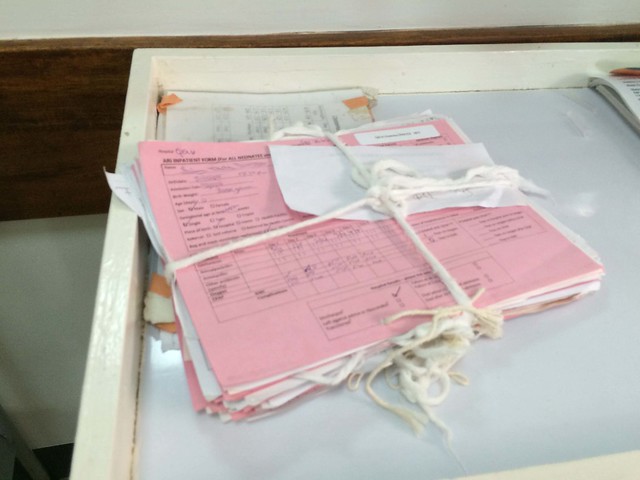
Once health passports are brought to hospitals, they’re incorporated into the medical charts for the patient. These charts include referral forms from other hospitals, basic information about the patient, surgical updates, doctors’ notes, and more. Since staples are at a premium here, gauze is used to hold the records together and the charts are usually placed wherever there is space (walls, sinks, hanging nails). Sometimes this leads to misplaced files in the hospitals. Karen and I talked to a few doctors and nurses about this problem and came up with the idea of putting laminated folders on the walls next to each patient bay as a chart holder. It’s an exceedingly simple solution, but we hope it will make the jobs of the doctors and nurses just a little bit easier. So far we’ve made one chart holder as part of a trial run and have seen a lot of excitement from the nurses in the ward, which hopefully means that we can start expanding this to more patient bays.
Records held together with gauze
Patient chart resting on the side of a hot cot
Chart holders may be a stopgap solution, but the bigger problem at QECH and other hospitals is the lack of storage space and organizational materials to help keep track of patient records. Already, nonprofits like Baobab Health Trust are encouraging longer term solutions–in Baobab’s case they do this by creating EMR systems out of recycled computers. At Queens we saw another newly implemented electronic system that creates international birth certificates for babies born in the hospital. The Malawian healthcare system has been fairly slow in the uptake of some of these electronic systems, but as momentum begins to build, telecommunication infrastructure improves, and computer literacy grows, it is increasingly likely that battered charts held together by tenuous ropes of gauze will become a thing of the past.
Blantyre is very much the pedestrian’s city. Many times throughout the day there are far more people walking on the streets than cars driving up and down them. With so much emphasis on walking around, I’ve found that the things I carry with me take on greater value. In these past three weeks, I feel like I’ve done a pretty good job of streamlining my backpack inventory. Here are a few of the essentials:
Camera – I’ve been averaging about ten pictures a day. The last ten or so pictures I’ve taken include snapshots from our walks to work, medical equipment from PAM and QECH, my lunch, people we’ve met, and some huge wasps that have been getting into our house the past couple of days.
Notebook and Pen – After just a couple of days, I realized I needed to buy a small notebook to write down all the Chichewa words and phrases I was learning. My Chichewa is still very rudimentary at best, but hey, ndikuphunzira!
Planner – With limited time here this summer and lots of things to do and people to meet, time management is a big challenge. My planner has been very useful in keeping up with all the meetings we schedule and for more long-term planning as we move into starting a few different projects.
Trusty Blue Jean Jacket – I came to Malawi straight from the steamy grip of Houston summer, so I foolishly thought that one blue jean jacket would suffice for the trip. To my surprise, it can actually get quite chilly here, and so my last-minute-luggage-addition has proven to be a daily and invaluable traveling companion.
Wristwatch – As far as I’ve seen, there are not very many clocks in Blantyre, and especially since the sun sets so much earlier than I’m used to in Texas, it’s very easy to lose track of time.
Emily’s Universal Power Strip – This is one I don’t actually carry, (Emily does,) but it has been an absolute lifesaver for our team. It’s a surge protector with a Malawian plug, but six universal outlets. That way, we can plug in all our American devices and any Malawian devices from one outlet and not have to worry about differences in voltages across devices or power surges from the wall.
And finally….
My Water Bottle – All the walking makes me thirsty!
The essentials minus the camera (used to take this picture) and the power strip (powering my laptop as I post this.)
In my fourth blog I wrote about our visit to PAM. Since then, the seven of us evaluated all of the different ideas for projects that we gathered there, and have developed a plan of action for the rest of the summer.
First, we talked about all of the observations we made at PAM until we could translate them into a list of potential projects. Then, we narrowed down that list to nine projects that we all thought could be feasible for the amount of time and people that we had to work with. From there, we each voted on our top 5 favorite projects to determine which ones we should pursue. It was really exciting to see that our favorite project had a unanimous vote of 7 and that the 2nd, 3rd and 4th place projects all still had a resounding majority vote.
Project
Priority (# of votes)
Estimated Duration (weeks)
Suction pump supplement to prevent overflow
7
3
Radial flow splitter
6
1/2
Platform to promote Poly/Rice student communication (probably website)
6
continuously
Constant temperature monitor for babies to prevent hypothermia, for hospital and at home use
5
2
Oxygen concentrator supplement or modification to promote less frequent breaking
3
—
Develop more communication channels between the Poly and their community in Blantyre
3
—
Bililight stands
3
—
Preventative maintenance plans for PAM
1
—
Autoclave supplement to prevent turning on the device before adding water
0
—
Based on our estimation of how long each project will take to complete, we have decided to pursue the suction pump, flow splitter, Poly/Rice website and temperature monitor. Already, we’ve put together a prototype of the flow-splitter from mostly locally available materials, and have started research for the suction pump project. In addition to the research we’ve been conducting online, today we stopped by PAM again to take a closer look at some of their broken suction pumps. The idea still needs development, but one promising lead is to attach infrared sensors externally to the collection jars so that when the liquid reaches the level of the sensor an alarm will sound and the pump will be turned off.
In other news, last week we spent a morning in the library helping Charles, Andrew, Christina and Francis set up their blogs. I added hyperlinks, so click on their names to read their latest posts!
This next week looks like it’s going to be pretty busy. One of the big things we’ll be starting is the design of some supplementary component to add to Queens hospital’s suction pumps, which break often. Suction pumps are used to drain fluids from the patient’s lungs, stomach, and throat. The problem we’re going to be solving occurs because nurses don’t have time to constantly monitor the suction pumps when in use. The pumps drain all waste into a large container, but when the container fills up beyond it’s capacity the fluids will start to enter the tubing that connects to the main device and motor. If the fluids get into the motor, the device breaks. Our team of electrical, biomedical, and mechanical engineers wants to create something that can be added on to an existing pump, so that either the fluids don’t have access to the motor, an alarm sounds to alert the nurse when the container is full, or both. I’m very excited about this challenge because it’s a unique one; we aren’t designing something completely from scratch, but instead we must lend our design to absolute compatibility with any suction pump found in Queens. We’ve started doing some basic research, and I think by the middle of the week we’ll have enough background on the issue to start thinking of design.
The other project we intend to get a good start on this week is a website that can be used for communication between Rice and Poly design teams. Sarah, Catherine and I were in such awe when we brought the Rice design projects in to show Charles, Christina, Andrew and Francis, and they immediately had great feedback about all the technology. Having a platform for direct contact between students would be valuable for design teams to have other perspectives on their devices. If communication was sustained, it would be personally valuable for each side because they would have a better understanding of what engineering is like across the globe. Francis and Sarah both have a lot of interest in starting this project off, and I have a little bit of background in website design that I hope will be helpful to them. We’ve set some pretty ambitious goals for this week, but I think there is so much enthusiasm and passion for the work that achieving them is well within our power.
Acquiring cell phones here was extraordinarily easy. We popped into a store located a ten minute walk from the Poly, and quickly obtained phones, chargers, and minutes all for 5,500MKW, or $12.22. Though we chose to buy the simplest phones, only capable of calling and texting (used for communication between the interns), there were also smart phones readily available for purchase. Users of all cell phones buy minutes and bandwidth on the street, from vendors who set up at small tables on almost every corner in downtown Blantyre. The entire process is run by immediate consumer need—users buy only the minutes they want, when they want them—which makes it adaptable. There are no formal bonds committing cell phone users to one supplier, and there are no wasted minutes nor wasted bites. Within Blantyre, access to the internet—and access to its world of information—through common cell phones is pretty widespread.
Internet access and cell phone usage across Africa has shot up in the past decade. Though both of these systems are still centered largely in the urban cities, they are beginning to penetrate further into rural areas. Like all expanding infrastructure, extending the digital network will take time, resources, and restructuring. However the speed that our technical abilities have grown to me indicates a promising near future in which the internet can be accessed at least by some in most areas of the world.
Even at Rice, there is currently research focused on, classes offered about, and programs aimed towards creating clever ways to expand internet access into low-resource areas. Discovering methods to reduce necessary additional physical infrastructure in order to drive down the price of internet while maintaining quality is an area of research where I see electrical engineering overlapping with the potential to improve global health.
Of course, in some instances, there is no feasible digital substitute for an in-person, trained doctor. In the ideal future, there may be an adequate number of capable health care workers to work on-site with patients; as it stands, however, the ratio of doctor to patient in much of Africa is far less than this ideal:
As a result, for every one physician in Zimbabwe there are 6,300 patients, and in Cambia, 9,300. In Ethiopia it’s 45,400 patients per physician, and in Liberia, it’s 71,400 to one. There are only 120 doctors and 100 nurses for the 11.3 million residents of South Sudan. (1)
Stable internet and a framework through which district hospitals and smaller health-care centers can interact with larger hospitals may provide a trusted channel for rural healthcare workers to communicate questions to and glean advice from specialized doctors in the city centers. While not ideal, such interactions may improve education and health care practices in the interim. There is also opportunity for increased efficiency. Trainings and updates that can be communicated over the web prevent excess time and resources from being spent. A quote from Wired magazine conceptualizes this potential:
Wires warp cyberspace in the same way wormholes warp physical space: the two points at opposite ends of a wire are, for informational purposes, the same point, even if they are on opposite sides of the planet. The cyberspace-warping power of wires, therefore, changes the geometry of the world of commerce and politics and ideas that we live in. (1)
Once this network is made accessible, interacting with it is quick and easy—just like our experience buying cell phones here. Supplying the internet is the hard part of this equation, but once present people of vastly varying ages and education levels will be capable of benefitting from it. The project of expanding Wi-Fi is incredibly complex, and is something that long-term (after much more schooling) I may look into pursuing. For the time being, though, we as interns can at least begin thinking about the various ways in which we can take advantage of this expanding network.
New devices for digital healthcare. For internet-enabled-healthcare to be feasible, current health technologies and practices have to be reimagined. For pictures and videos to transmit information from a patient to a physically distant doctor, we must find alternative ways to communicate accurate information about attributes such as size and color of objects that, in person, are taken at face value. This is a problem that a recent Rice global health team tackled. In Barretos, a cancer hospital has nurses take photos of patient skin lesions across southern Brazil, then send these photos in to the central hospital. A doctor then evaluates these photos to determine if the patient should make the trip to the hospital for further evaluation. The device is a physical attachment to cell phones which improves color and size interpretation, as well as photo clarity. Two Rice BTB interns are in Barretos this summer, rolling out the new technology—if you are curious and want to learn more, check out Pablo or Megh’s blog!
Development of communication channels. I wrote a post about the importance of collaboration before, and access to Wi-Fi facilitates the development of these relationships. Looking forward in this internship, one of the projects we hope to pursue is creating a system to connect Polytechnic students with Rice students; this connection has the potential to benefit both academic growth as well as device success. Almost any two institutions involved in my global health experience so far could benefit from increased communication, resulting in rising rates of both efficiency and efficacy.
Preventative maintenance. During our tour of PAM last week, we noticed many of the devices suffered a malfunction caused by user error. Considering the array of machines that fills hospital wards, it isn’t surprising that small user mistakes are frequent. Even more frequent is forgotten technology maintenance: some devices require a new filter every 2 months, while other devices require lubrication every week, still others require water to be kept at a steady level throughout use, and others require constant monitoring for overflow. The intricacies of every device can get overwhelming even for maintenance engineers, and far more so for busy nurses who have patients to attend to. Sometimes, simple check-ins with the trained employees at PAM could prevent major device breakdown. However, as I’ve mentioned before, PAM does not have the funding to visit various district hospitals for preventative maintenance needs. There are many possibilities that can be explored to decrease device misuse/overuse by establishing a live connection between engineers and the smaller healthcare centers. For example, technology-specific overview videos could be created to remind nurses of common user interface problems and required maintenance needs; training updates for new practices could be conducted over the web, or forums created for common questions. All of these channels would need to be streamlined and organized, however they again provide the potential for increased efficiency and efficacy.
Of course, the expansion of internet has far greater implications than just healthcare, and the adoption of these new, Wi-Fi enabled technologies may meet some huge barriers. Users would need to adapt to a new method of communicating and working, as computer technology brings in its own learning curve that could slow progress. However, since internet usage rates are already on the rise, a new market full of largely untapped possibilities is coming regardless; it only makes sense to begin reconsidering past solutions to present problems.
Taking photos of the finished dosing meter to send to friends over textWorking on blogs, which are one example of how the internet is helping us to form cross-continent global health connectionsTypical day at work, surrounded by desktops, laptops, and cell phones used to GoogleOne of the many AirTel stands in Blantyre, where minutes are easily bought.
(1) Olopade, Dayo. The Bright Continent: Breaking Rules and Making Change in Modern Africa. N.p.: First Mariner, 2015. Print.
When I was growing up, my dad’s trivia was a staple of any gathering. Be it a birthday full of screaming 8 year olds, a family gathering, or dinner party, it wasn’t truly a Wettermann event until Dad pulled a trivia printout from his back pocket. He has this uncanny ability to find some vaguely relevant topic to quiz us on. Competition ran high. Details were scrutinized. Egos were bruised.
It was awesome.
Although I’m waaaaaaaay too far from Chicago to compete in Bob Wettermann’s world famous* trivia, my dad’s games have still left their mark. So what better way to celebrate Father’s Day than to challenge you, dear reader, to this time honored tradition? Without further ado, here’s some Malawian trivia in the spirit of the world’s best dad:
Which of the following colors is NOT featured on Malawi’s flag?
a. red
b. yellow
c. green
d. black
Before independence from the UK in 1964 by which name was Malawi known?
a. Queensburg
b. Chewaland
c. Nyasaland
d.Blantyre
What product accounts for over 50% of all Malawi’s exports?
a.Tobacco
b.Tea
c. Maize
d.Cotton
Which is the currency of Malawi?
a.Malawian shilling
b.Malawian goude
c.Malawian bwanji
d.Malawian kwacha
How many districts are there in Malawi?
a. 7
b. 16
c. 28
d. 41
The most common Malawian last names are Chirwa, Banda, Piri, and Manda. What percentage of the country’s inhabitants have one of these surnames?
a. 15%
b. 30%
c. 45%
d. 50%
What food do most Malawians consume at least once daily?
a. Sugar cane
b. Tomatoes
c. Maize flour
d. Carlsburg beer
Malawi is roughly comparable in size to which US state?
a. Pennsylvania
b. Illinois
c. New Jersey
d. Delaware
*Disclaimer: probably.
My dad and me in Les Cayes, Haiti- it was both of our first times experiencing service in the developing world. He has been endlessly supportive of my passion for global health since then. I can’t imagine a more loving or caring encourager!


 2:00PM-5:00PM- More meetings, and working on Morphine Tracker.
2:00PM-5:00PM- More meetings, and working on Morphine Tracker.